Introduction
Xylitol was first discovered by Emil Fisher, a German chemist, et al. in 1891 [1]. As it became possible to commercially produce xylitol by adding hydrogen to xylose extracted from plants in 1960s, it started to be used to produce foods as a sweetening agent [2,3]. Then, a research team led by professor Mäkinen of Turku University in Finland proved xylitol's dental caries prevention effect [4,5], and thus xylitol was internationally approved as a functional food that can reduce a risk of dental caries. Now xylitol is being made and distributed in various forms, including gum, candies, snacks, syrups, tablets, etc. [6].
Xylitol is highly recommended in the dental health field and is becoming more commonly and positively recognized by the public. However, most people do not know the exact mechanisms of dental caries prevention based on detailed grounds or data, and even are not aware of an exact method to use xylitol. Dental health specialists who provide common people with dental health knowledge just simply promote xylitol's positive images, without informing of exact effects and an appropriate method to use it [7]. According to a study on dental health specialists' awareness of xylitol's dental disease prevention effect, dental hygienists and dentists showed comparatively low awareness with respect to xylitol, and had even partially wrong knowledge about it [7]. It is because, although there have been many types of research proving xylitol's dental caries prevention effect, the results were very confusing since daily intake amount, intake times, intake periods, etc. are not consistent, assessment index is too various - the number of dental caries-causing bacteria in the mouth, acid concentration of saliva and dental plaque, the amount of dental plaque, dental caries occurrence rate, etc. - , and sometimes research results were different depending on the kinds of assessment index, form of xylitol and intake method. In particular, most xylitol products currently being sold are mostly mixtures of xylitol and sugar, without complete exclusion of sugar. Thus, the dental caries prevention effect of such products may differ depending on the content of xylitol [8]. In research by Barber et al. [9] published via Journal of the American Dental Association, an official journal of the American Dental Association, 691 adults consumed in total 5 g of xylitol over 5 occasions a day for 33 months. As a result, the xylitol group showed 10% decrease in dental caries increase rate compared to the control group. However, since it failed to reach 1/3 of the total number, the researchers considered that the result is statistically insignificant and decided not to present it. Therefore, in order to claim xylitol's dental caries prevention effect, it is needed to systematically examine researches that have been published and objectively assess xylitol's effect. Thus, this study intends to provide with an effective method to use xylitol by collecting previous studies proving xylitol's dental caries prevention effect and analyzing and classifying their features.
Text
1. Reference search and selection
In this study, various studies on xylitol published by domestic and international journals were collected and analyzed. Foreign documents were searched via MEDLINE (PubMed) and Google Scholar, and domestic studies were found via domestic databases such as RISS, KISS, and the National Assembly Electronic Library. Key words used for search were ‘xylitol’ and ‘caries’ in Korean, ‘xylitol’ and ‘caries’ in English, and a combination of the words. Via first search, in total 612 documents were found: 27 domestic and 585 international studies. After excluding duplicate documents and theses, 146 documents were left. Among them, 94 clinical studies in which xylitol was directly applied to a human body were analyzed <Table 1> [4,5,9-100], and double counting was selected to analyze the documents.

2. Characteristics of the research methods in studie
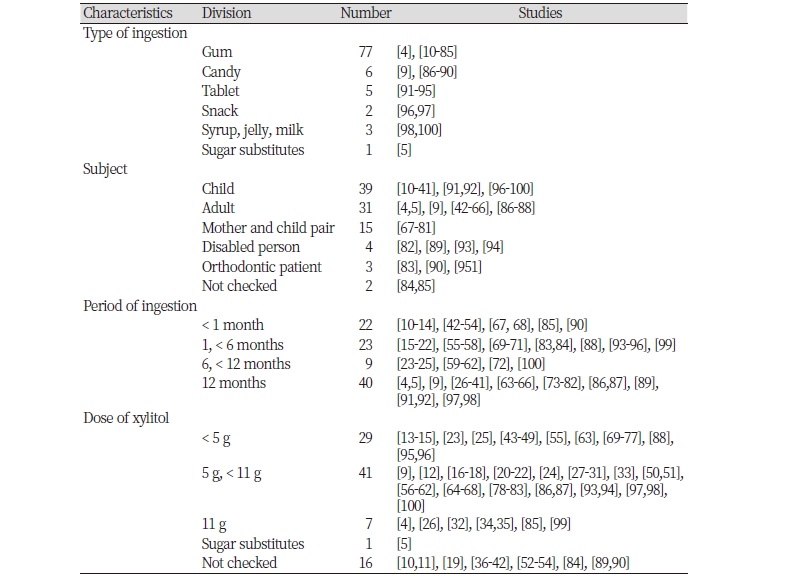
Having compared characteristics of clinical researches where xylitol was directly applied to human bodies, the most commonly used form of xylitol was gum, which was used in 77 researches, followed by candies and tablets, which were respectively used in 6 and 5 researches. Snacks were used in two researches, and syrup, jelly, and milk were found in one research respectively. Also, there was one research where sugar was completely replaced by xylitol.
In terms of targets, young children and elementary school students, studied in 39 researches, were most common. The second most common target was adults, found in 31 researches. There were 15 researches carried out in pregnant women and pairs of mothers and their young children in order to verify the effect of preventing mother-to-child transmission of caries-causing bacteria in the mouth. Also, 4 and 3 researches respectively studied the disabled and orthodontic patients with high risk of dental caries. There were two studies of which targets were unclear because they did not specify the ages of the targets <Table 2>.
Having analyzed consumption period, 40 researches were carried out for at least one year. Then 9 were performed for at least 6 months and less than 12 months, 23 were for at least one month and less than 6 months, and 22 were for less than one month. That is, many researches tended to be carried out for a long period. The most common consumption amount was at least 5 g and less than 11 g, followed by less than 5 g and then at least 11 g. There were also many cases where the amount of xylitol was not specified <Table 2>.
3. Index for evaluating xylitol's dental caries prevention effect
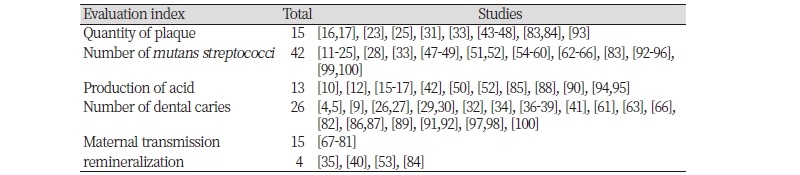
Having analyzed, via double counting, indexes used to evaluate dental caries prevention effect that occurs after xylitol intake, the most commonly used index was the change in the number of caries-causing bacteria, in particular muntans stretococci (MS), in the dental plaque or saliva, followed by caries occurrence rate, maternal transmission, acid production, the amount of dental plaque, and remineralization. In most studies, each evaluation index decreased after xylitol consumption. However, in some researches there were no remarkable changes in evaluation indexes <Table 3>.
4. Characteristics of references which are negative to xylitol's dental caries prevention effect
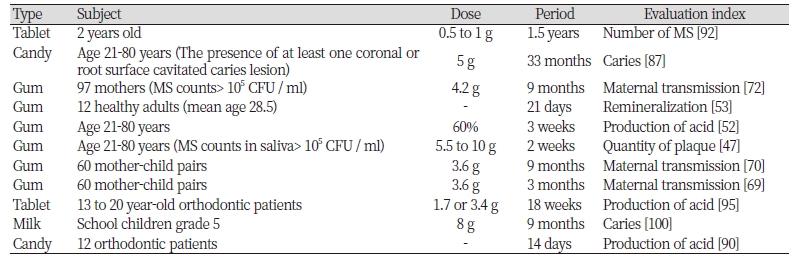
In total 11 studies stated that xylitol's effect was not found in at least one of the evaluation indexes. Characteristics of each research are explained in <Table 4>. It is notable that most of the researches used less content of xylitol or were carried out in a shorter period, compared to other researches. Some studies failed to find significant effect of xylitol although comparatively high content of xylitol was consumed for a long period. However, such a result was caused because the form of xylitol taken in the studies - milk, etc. - stayed for a very short time in the mouth compared to other forms.
5. Summary of xylitol’s dental caries prevention effect
1) Reduction of dental caries-causing oral bacterium
Healthy children who masticated xylitol gum for 6 months or at least one year showed significant reduction in mutans streptococci (MS), a dental caries-causing bacterium, in dental plaque [23-25,28]. Even those who masticated xylitol gum for a comparatively shorter period, such as 1 month or less, showed significant decrease in MS. The number of MS in the mouth also decreased, regardless of the intake period and consumption amount, in children with comparatively high concentration of MS in dental plaque or saliva or with positive regions of dental caries, or children wearing orthodontic appliances and thus having a high risk of dental caries. In studies carried out in adults, the number of MS in the mouth was significantly cut down in those who masticated xylitol gum, regardless of the period, despite the wide age range and various mouth conditions.
In addition, studies in which xylitol were consumed in the form of milk and jelly resulted in significant decrease in the number of MS. In one case, elementary school students (1st to 5th grade) consumed xylitol-containing jelly three times a day (in total 15.6 g/day) for 6 weeks. In another case, such students consumed 8 g of xylitol-containing milk per day for 9 months. The number of MS in the mouth decreased in both cases [99,100]. In researches where xylitol tablets were used, adults showed significant reduction in MS [93-95]. However, in a study where young children consumed 0.5 to 1 g of tablet per day, decrease in the number of MS was not found [92]. It is assumed that such difference of results was caused not by the age difference but by the consumption amount of xylitol.
2) Decrease in dental plaque
In one research, 28 adults of average age 22.5 masticated gum containing xylitol (10.9 g/day), sorbitol (10.9 g/day), xylitol+sorbitol (8.5+2.4 g/day), and sugar. They consumed two pieces at once and 5 times a day, for 2 weeks. As a result, the amount of dental plaque was reduced by 24.3% in the xylitol+sorbitol gum group and by 29.4% in the xylitol gum group [46]. In a similar study, adults (18 years old or older) masticated xylitol-containing gum (4.25 g/day) for 2 weeks. As a result, their dental plaque significantly decreased [66]. On study had dental school students stop dental care activities and instead consume gum containing mixture of sorbitol and xylitol (1.6 g of sorbitol/day; 8.7 g of xylitol/day), and another study had students (age 23-25) masticate xylitol gum for two weeks. Both groups showed decreased accumulation of dental plaque compared to the control groups [45,48].
It was found that xylitol has effect not only to adults but also to children. In one study in which 13-15 year-old children masticated xylitol-containing gum 5 times a day (10 g/day) for 4 weeks, the dental plaque index was significantly reduced compared to the control group [17]. In a study carried out in younger children (age 10), those who masticated xylitol-containing gum for 40 months showed a lower index of dental plaque compared to the control group [31]. However, one study failed to find any decrease in dental plaque although targets masticated xylitol gum 3 to 5 times a day (5.5 to 10 g/day). The study was carried out in 18 to 29 year-old adults whose saliva contain MS of 105 CFU/ml, so the targets had a higher risk compared to other studies. Although the dental plaque of the targets was not decreased, the number of MS in the mouth was reduced.
3) Decrease in acid production
Acid production in the mouth is roughly divided into acid production in the saliva and that in the dental plaque. In children who masticated xylitol gum for 4 weeks, acid production in the dental plaque decreased or the lactic acid concentration in the saliva significantly decreased [16,17,33,56]. The lactic acid concentration in the mouth was reduced by 22% even in children who masticated xylitol gum (5 g/day) for a comparatively shorter period of 2 weeks [12]. Even those who masticated xylitol gum only once for 10 minutes showed significant increase of pH in their dental plaque [10]. In a study carried out in adults, the group that masticated xylitol gum for 2 weeks showed higher pH in the dental plaque than the groups masticated sugar gum and sorbitol gum [50]. The group that consumed xylitol candies (2 g/day) for 4 weeks also showed higher pH in the mouth than the sorbitol group [88].
However, according to Stecksén-Blicks et al. stated that. although orthodontic patients (age 13-20) who consumed xylitol tablets 2 or 4 times a day (1.7 g or 3.4 g) showed decreased acid production, the degree of decrease was not significant compared to the control group [95]. Also, a study which had students (age 20-30) masticate xylitol gum for 3 weeks reported that the pH of their saliva did not significantly increased [52]. In addition, in a study which had orthodontic patients consume xylitol candies 5 times a day for 14 days, the minimum pH of the dental plaque rose from 4.81 to 5.09, but the final pH of the dental plaque was not significantly different from that of the control group [90].
4) Reduction of dental caries occurrence rate
When 10 year-old children who consumed xylitol (5 g/day) in the form of gum or candies for three years, their dental caries occurrence rate significantly decreased, by 35 to 60%, compared to the control group [27]. In case of elementary school students (age 11-12) who masticated xylitol gum (10 g/day) for two years, their DMFT increase rate was inhibited by 45%, and the greater amount of xylitol consumption led to better dental caries prevention effect [30]. In one study, 274 children (age 8-9) were divided into a 15% xylitol gum consumption group, a 65% xylitol gum consumption group, and a control group, in order to verify xylitol gum's effect on dental caries's occurrence and progress. As a result, the group that consumed gum showed significantly lowered progress of dental caries, and the two gum-consumed groups had similar results [41]. In another study, 1,277 children were divided into 8 groups: 4 xylitol groups (4.3 to 9.0 g/day), two xylitol/sorbitol groups (polyol 8.0 to 9.7 g/day), one sorbitol group (9.0 g/day), and one sugar group (9.0 g/day). Having compared their dental caries occurrence rate after the children masticated the allocated material for 40 months, it was found that 100% xylitol gum was most effective to reduce dental caries occurrence rate [29]. When DMFS according to substitution of sugar with xylitol and fruit sugar was compared, the group that consumed sugar resulted in 7.2, the fruit sugar group resulted in 3.8 and the xylitol group resulted in 0.0, proving that xylitol consumption decreases dental caries occurrence [5]. Further, dental caries occurrence rate of those who masticated xylitol gum was not significantly different from that of those with sealants [36]. However, those who consumed xylitol-containing milk (8 g a day) for 9 months did not show any decrease in dental caries occurrence [100].
5) Promotion of remineralization
In a study, 10 or 6 year-old children masticated xylitol, sorbitol or xylitol-sorbitol gum for 40 months or 24 months respectively. When compared to those who did not masticate gum or masticated sugar gum, the groups that masticated xylitol/sorbitol gum showed prevalent remineralization in permanent teeth after 40 months and in milk teeth after 18 months. In addition, the group that consumed 10 xylitol candies a day (maximum xylitol 20 g/day) had strengthened enamel hardness and promoted remineralization compared to the group that did not consume xylitol [35].
When the content of calcium in dental plaque was compared, it was found that mastication of xylitol and sorbitol gum for 6 weeks not only inhibits accumulation of dental plaque but also strengthens remineralization [84].
6) Inhibition of mother-to-child transmission
In one study, 195 pregnant women with high number of MS in their saliva (≥105 CFU/ml) were divided into a group of having xylitol-containing gum (65%) 4 times a day (xylitol 6 to 7 g/day) for 3 to 21 months and control groups of a fluorine-applied group and a chlorhexidine-applied group. As a result, when their children became 3 years old, MS was found in 27% of the xylitol group's children, 64% of the fluorine group's children, and 37% of the chlorhexidine group's children. That is, it was verified that regular mastication of xylitol gum by mothers can reduce transmission of MS to children [67,68,79]. In addition, having traced and studied the above targets for the next 10 years, it was found that children of the group in which mothers masticated xylitol did not have any dental caries until 8.2 years old, which is very high compared to that of the control group (5.8 years old) [78]. In a similar study, pregnant women with comparatively high number of MS in their mouths masticated xylitol gum 4 times a day (in total 5 to 10 g of xylitol a day) for 13 months. Children of the xylitol group were infected by MS at a comparatively older age than the control group [80]. In a large scale carried out in mothers in Sweden, when mothers masticated xylitol gum (xylitol 1.95 g/day) three times a day for 1 year, their children showed low dental caries occurrence when they became 3 to 4 years old compared to the control group. The children's MS was similar to the MS of children of mothers whose MS in saliva is low [73-76].
In a study carried out not in pregnant women but in mothers with children, it was also found that mastication of xylitol gum (xylitol 1.8 g/day) can reduce MS transmission to children, resulting in low MS index in the children's mouth as well as low dental caries occurrence rate, which was 6 times higher in the control group [77,81].
Meanwhile, some researchers reported that mothers' xylitol consumption does not have any effect of inhibiting dental caries of their children. According to Fontana et al., although mothers masticated xylitol gum 3 times a day (xylitol 4.2 g/day) for 9 months, there was not any significant difference between the xylitol group's children and the control group's children in terms of the number of MS in their mouth and microorganism composition in their dental plaque [72]. Children of mothers who masticated xylitol gum (3.64 g/day) for 3 months did not show difference in terms of the number of MS in the mouth and DMFT compared to those before experiment, and their dental plaque index was not different from that of the control group [69].
Conclusions
Having analyzed and compared previous studies, it was found that most researches that applied xylitol's dental caries prevention effect to human bodies concluded that xylitol is effective for preventing dental caries, and they provided the following grounds: decrease in the number of MS in the mouth; decrease in the quantity of dental plaque; reduction of pH in the mouth; inhibition of mother-to-child transmission; and remineralization effect. The most precise way to verify xylitol's direct effect of dental caries prevention is to check decrease of dental caries occurrence in the mouth. However, the number of studies directly showing a decrease in dental caries occurrence rate is less than those using other indexes. Thus, further study in this matter is needed. Nonetheless, many studies positively evaluated xylitol's effect, albeit indirectly and thus it can be concluded that xylitol is helps reduce the risk of dental caries.
The reasons why xylitol is effective for dental caries prevention are explained as follows: First, xylitol increases saliva secretion through organoleptic stimulation. Then, the pH of dental plaque rises, thereby preventing enamel from demineralization and causing its mineralization [101]. Second, xylitol's chemical structure makes it act with polyvalent ions such as calcium and form a stable complex, thereby contributing to stabilization of calcium phosphate in the dental plaque. Third, xylitol increases concentration of amino acids and glycin in saliva; saliva proteins in the parotid and the palatal gland; operation of amylase; carbonic anhydrase, lactoperoxidase, invertase-like enzymes, thioxyanate ions, etc. These changes in saliva components augment saliva's buffering and bacteriostatic effects, thereby enhancing the body's defense mechanism against dental caries [102-104]. Fourth, xylitol is accumulated in cytoplasm of Streptococcus mutans (S. mutans), a representative caries-causing bacterium, in a non-metabolic form of xylitol-5-phosphate (X5P) and then inhibits vitality of enzymes related with glucose metabolism, discharges from cells, brings back into cells, and repeats the above process. Through the futile cycle of consuming energy, xylitol can inhibit proliferation of bacteria [105,106].
11 of in total 94 documents reported at least one non-positive result regarding xylitol's effect, and only 4 documents claimed that it was not effective at all. Compared to other studies which are positive to xylitol's effect, these researches used a smaller amount of xylitol or were carried out for a shorter period. Therefore, the consumption period and consumption amount are considered to be very important factors in confirming xylitol's effect. Having analyzed the documents, it is considered that xylitol can show dental caries prevention effect when it is consumed at least 5 g a day for at least one month, and the larger consumption amount and the longer period can bring about a better effect. Although an increased consumption amount and consumption period can lead to a greater expected effect of xylitol, reports on xylitol's safety suggested that consumption of excessive amount of xylitol may cause diarrhea [107,108]. In addition, considering xylitol's raw materials, an appropriate maximum amount to consume should be studied in order to achieve dental hygienic enhancement of all people including children. According to studies on xylitol's safety and researches in children, the daily maximum consumption amount is estimated as 25 g [107-109]. However, since 5-11 g of xylitol is sufficient to show the dental caries prevention effect, it is deemed that its appropriate consumption amount is 5-11 g. The American Dental Association recommends 5 to 8 g of xylitol as an appropriate consumption amount [110], and Edgar and Geddes [111] reported that 6 to 12 g is an appropriate consumption amount.
Researches in which xylitol showed insignificant effect have a common feature regarding the dosage form of xylitol. These studies used xylitol in a dosage form of milk etc. which stays in the mouth for a very short time. Xylitol should stay for a long time in the mouth in order to show significant effect. To this end, it is preferable to take xylitol in the form of a candy or tablet which is slowly melted in the mouth, rather than milk or syrup that is swallowed at once. The American Dental Association also recommends to take xylitol in the form of a candy or tablet after having a meal [110]. Further, according to Jeong et al. [7], when xylitol in the form of tablet is more effective when it is slowly melted in the mouth rather than when it is chewed. Xylitol gum is also another good choice to have xylitol stay for a long time in the mouth. Mäkinen et al. [32] reported that pellet-type gum is more effective than chewing sticks. Further, having examined various documents, it was found that most researches that had targets masticate xylitol-containing gum reported xylitol's positive effect of preventing dental caries.
Having analyzed evaluation indexes used in the documents which failed to find xylitol's positive effect, 4 indexes showed similar distributions to each other, while there was one document which did not check the number of MS in the mouth. Thus, it can be said that xylitol is very effective to reduce the number of MS in the mouth. In particular, since the document used only 0.5 to 1 g of xylitol, it is considered that the lack of effect was caused by the low consumption amount. Thus, an appropriate amount of xylitol will be able to effectively inhibit MS in the mouth.
The most common targets of the analyzed studies were young children and elementary school students who have a high risk of caries. There were also many studies in adults, and some were carried out in the disabled and orthodontic patients with a high risk of caries. There was not any difference depending on the targets of the studies. Therefore, it is deemed that xylitol can reduce dental caries occurrence in all people, regardless of age or gender or the risk of dental caries they originally had.
In consideration of the above results, it can be concluded that consumption of 5 to 11 g of xylitol in the form of gum, candies, or tablets for a long period is useful to reduce risk of dental caries. In addition, xylitol can be easily consumed by any people, regardless of gender or age, and even by children and the disabled who have difficulty in dental care. Therefore, dental health specialists should obtain precise knowledge about xylitol and learn an appropriate consumption method so as to provide specific and precise information to the public and promote xylitol to them such that many people can effectively use xylitol. There is a limitation that this study focused mainly on the analysis of research forms in clinical studies only and that the analysis of results in literature was not performed in close detail. Further, it is considered that more concentrated and multilateral studies on an appropriate time to start to consume xylitol, consumption frequency, an appropriate dosage form to maximize xylitol's effect, etc. should be carried out in the future.

