Introduction
Strict consideration of hand hygiene is an essential aspect of patient protection and also of safeguarding of dental workers’ safety as dental care settings are often widely exposed to various pathogenic microorganisms[1]. Numerous studies conducted in Korea reveal lack of compliance by medical practitioners as many of them do not wear gloves[2] due to discomfort or simply because their co-workers choose not to and this lack of awareness often functions as a major obstacle to hand hygiene[3].
In dental health care settings, pathogens can be transmitted through patients’ skin, dental workers’ hands or cross contamination of various organisms[4]. Among viruses that dental hygienists are often exposed to during standard dental hygiene care procedures, hepatitis B virus found under participants’ nails survived more than 7 days at room temperature in a particular study[5]. Slower bacterial growth and more precise or effective hand washing are observed in individuals with shorter nail lengths compared to individuals with longer nails[6]. Moreover, studies suggest that accelerated bacterial growth is detected in nails longer than 2 mm and nails longer than 3 mm reportedly show 6 times higher likelihood to carry gram-negative Pseudomonas aeruginosa compared to shorter nails[7].
When medical gloves are worn on manicured hands, normal microbial flora multiply 4,000 times faster and more complexly in the moist environment underneath gloves[8]. Furthermore, patients could be exposed to various pathogenic bacteria due to invisible tears on gloves which could pose a greater threat to patients with weak immunity. Moreover, risks of infections due to gram-negative bacteria such as Pseudomonas aeruginosa, Serratia marcescens and candidas[3].
Various forms of “nail art” including manicure and artificial fingernails worn by dental workers are not recommended in most infection control guidelines in dental settings[9]. On the contrary, maintaining short fingernails is recommended among such individuals[10]. However, as the popularity of applying manicure, artificial fingernails or other fashionable decorations has increased recently, these so-called “nail art” experiences in dental hygienists could also be increased compared to before. An online survey of 1,000 participants in Korea revealed 66.5% of nail art experience rate[11], which validates the significance of concerns in the field of dental hygiene regarding the trend. “Nail art” means painting on long nails, including manicure, or attaching beads or jewelry.
Maintaining hand hygiene, which is an essential basis of infection control principles for all personnel working in medical institutions, has been treated as an important aspect for patients and health practitioners, therefore numerous studies have been conducted regarding the subject[12,13]. Dental workers’ hand hygiene has been a popular topic in the field and it has been investigated through studies such as a study of hand hygiene practices in dental workers[2], a study of dental hygienists’ hand-washing before and after patient care[14], infection control via hand hygiene practices among dental hygienists[15]. Jung[16] reported through her study conducted on nurses that stronger behavioral, normative and control beliefs resulted in more positive dental hygiene practices .
Nail hygiene is a sub-concept of hand hygiene which is expected to be demonstrated through more frequent hand hygiene behaviors in individuals with stronger hand hygiene beliefs. Hence, the main objective of this study was to investigate current status of dental workers’ nail hygiene behaviors and the relationship between hand hygiene beliefs and nail hygiene behaviors.
Methods
1. Subjects
Dental workers including clinical dental hygienists working full-time at dental clinics, dental hospitals, general dental hospitals and dental university hospitals in Seoul, Gyeonggi-do and Incheon were randomly chosen for survey from June 21st to September 17th, 2016. Among these individuals, only those 329 people who showed understanding of the purpose and context of this study were given the survey questionnaire and 291 participants were included for the final analysis after excluding individuals with incomplete or erroneous answers.
The current study’s sample size was determined utilizing G*power 3.1 program. When the number of explanatory variable for univariate analysis was set at 3, significant level (α) at 0.05, power at (1-β) at 95% and effect size at 0.25, respectively, the appropriate sample size was determined to be 252 while that of one-group linear regression analysis was 270.
This study was approved by 00 University Bioethics Committee’s Institutional Review Board (Approval number: CR316016).
2. Instruments
For the purpose of this study, parts of a master’s thesis by Jeong[17] were re-analyzed and summarized. A structured survey questionnaire consisting of general characteristics and characteristics associated with hand hygiene beliefs and nail hygiene behaviors was used for the study. The survey questionnaire from the study by Jung[16], which was developed by translating and reverse translating the tool from questionnaire on hand-washing behavior by Whitby et al.[19], was modified for this study while questionnaire items regarding nail hygiene behaviors were newly developed based on previous studies. The questionnaire used in this study consisted of a total of 35 items; 4 items related to general characteristic, 25 items related to hand hygiene beliefs (12 items for behavior beliefs, 9 items for normative beliefs and 4 items for control beliefs), 2 items related to manicure or other forms of“nail art”experience and 4 items for nail hygiene behaviors[17].
3. General characteristics
The subjects’ age ranged from 20 to 56 years, with an average age of 28.2. Subjects’ job titles consisted of 4 areas; dental hygienists, dental assistants, dental coordinators and others which were categorized as dental hygienists and other dental workers for analysis. Clinical experiences of study subjects were analyzed by dividing into quartiles; less than 2 years, more than 2 years and less than 4 years, more than 4 years and less than 8 years and finally, more than 8 years. Work settings were categorized into dental clinics, dental hospitals, general dental hospitals and dental university hospitals.
4. Hand hygiene beliefs
Hand hygiene beliefs were categorized into behavioral, normative and control beliefs and were conveyed through a 6 point scale; strongly disagree (1 point), generally disagree (2 points), somewhat disagree (3 points), somewhat agree (4 points), generally agree (5 points), and strongly agree (6 points)[19]. Positive answers were taken as they were while negative answers were analyzed after reverse coding. The items that were reverse coding were two items: participation in dental care after nail application, maintenance of nail polish for more than 4 days.
The behavioral beliefs consisted of 12 items which were based on the belief in the positive effects of hand hygiene and showed reliability coefficient of 0.827. The normative beliefs consisted of 9 items which were based on the belief in other’s expectation of hand hygiene behaviors and showed reliability coefficient of 0.948. Lastly, the control beliefs consisted of 4 items which were based on the belief in the efficacy of hand hygiene behaviors and showed reliability coefficient of 0.719. In summary, all three types of beliefs demonstrated relatively high levels of reliability.
5. Nail hygiene behaviors
Questions regarding nail hygiene status of dental workers consisted of previous experiences with any forms of “nail art” current status of nails in terms of “nail art” application and the duration of such application, and whether or not each individual has had such experiences over the last 2 years or currently have “nail art” on by simple yes or no questions. Questions regarding each participant’s nail hygiene behaviors consisted of 4 questions (participation in dental care after nail application, maintenance of nail polish for more than 4 days, cutting when nail length is over 2 mm, keeping nail length within 0.5 mm); 2 negative questions and 2 positive questions, each with a 6 point scale, which demonstrated greater positivity with respect to greater final scores. Scores from the 4 questions regarding nail hygiene behaviors were used after converting into averages, and the reliability coefficient was 0.721. The sample sizes were shown to be different by items as answers with missing values were excluded.
6. Statistical analysis
Relationships between participants’ general characteristics and hand hygiene beliefs, their general characteristics and nail hygiene behaviors were analyzed via independent t-test, one-way ANOVA and Chi-square test, while the relationship between hand hygiene beliefs and nail hygiene behaviors was analyzed via pearson correlation analysis and multiple linear regression analysis. Statistical analysis was performed via PASW Statistics 19 with a statistical significance of 0.05 and a confidence interval of 95%.
Results
1. Relationship between dental workers’ general characteristics and hand hygiene beliefs
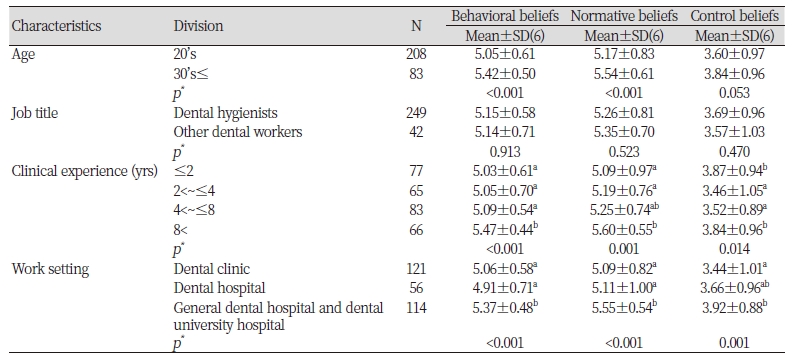
Significant differences were detected in behavioral beliefs and normative beliefs with respect to participants’ ages and in all of behavioral, normative and control beliefs in terms of participants’ clinical experiences and types of work settings(p<0.05). Among general characteristics that showed significant differences, behavioral and normative beliefs were slightly higher in individuals in their 30’s or older compared to participants in their 20’s. In terms of clinical experiences, behavioral and normative beliefs were the highest in subjects with more than 8 years of experience, while control beliefs were the highest in individuals with work experience less than 2 years. Interestingly, all three types of beliefs were the highest among individuals working in general dental hospitals and dental university hospitals <Table 1>.
2. Relationship between dental workers’ general characteristics and nail hygiene behaviors
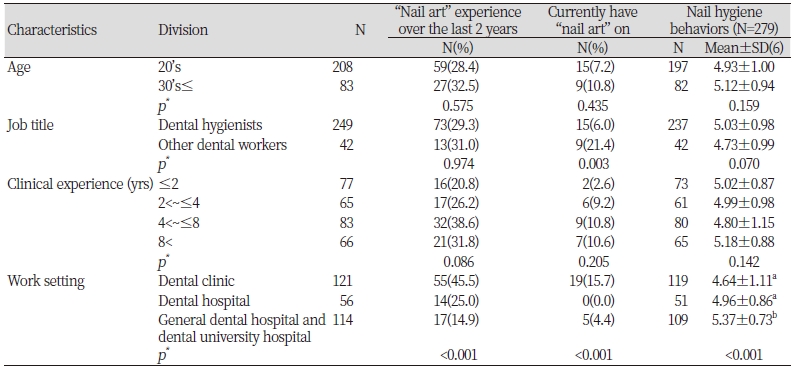
Significant differences were detected in subjects who currently have “nail art” on or who had related experience within the last 2 years and in nail hygiene behaviors with respect to work settings(p<0.05). Interestingly, participants who currently have “nail art” on or had related experience within the last 2 years were more likely to be working in dental clinics and the likelihood of practicing regular nail hygiene behaviors was the highest among individuals working in general dental hospitals or dental university hospitals, while that of individuals working in dental clinics was the lowest <Table 2>.
3. Correlation between dental workers’ hand hygiene beliefs and nail hygiene behaviors
The highest correlation was detected between behavioral beliefs and normative beliefs (r=0.605, p<0.01). Significant positive correlations were detected in nail hygiene behaviors with respect to behavioral beliefs (r=0.313, p<0.01), normative beliefs (r=0.307, p<0.01) and control beliefs (r=0.213, p<0.01) <Table 3>.
|
Table 3. Correlation between dental workers’ hand hygiene beliefs and nail hygiene behaviors (N=279) 
|
|
|
***p<0.01 by pearson correlation analysis |
|
4. Relationship between dental workers’ hand hygiene beliefs and nail hygiene behaviors
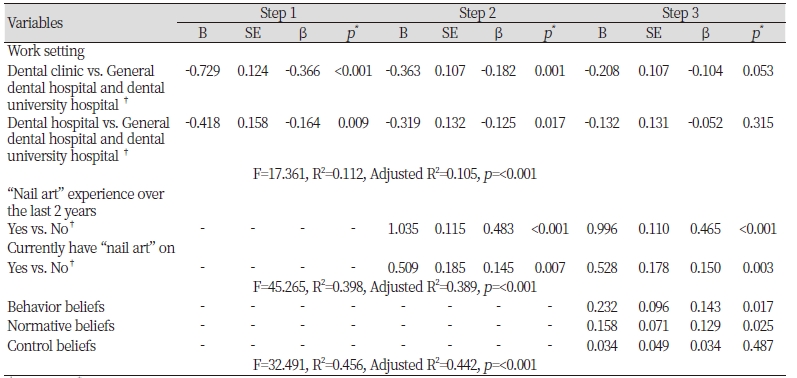
When all variables were analyzed via 3 steps with respect to nail hygiene behaviors, multicollinearity was not detected (VIF<10). The explanatory power from the first step in terms of nail hygiene behaviors and significant general characteristics was 10.5% with more lesser nail hygiene behaviors in participants working in dent al clinics compared to participants working in general hospital dental clinics or dental university hospitals. The prevalence of nail hygiene behaviors in participants working in dental clinics was slightly lower than general hospital dental clinics or dental university hospitals. When nail hygiene behaviors and general characteristics, “nail art” experiences were applied simultaneously for the second step, the explanatory power increased by 28.4% point and statistically significant differences were detected(p<0.05). When nail hygiene behaviors and general characteristics, hand hygiene beliefs, “nail art” experiences were applied simultaneously for the third step, the explanatory power increased by 5.3% point and statistically significant differences were detected(p<0.05). Nail hygiene behaviors were more likely to be observed in individuals with less “nail art” experiences over the last 2 years or now and also with greater behavior and normative beliefs<Table 4>.
Discussion
The objective of this study was to analyze the relationship between hand hygiene beliefs and nail hygiene behaviors among dental workers. Among such hand hygiene beliefs, control beliefs (3.69±0.96), which focus on individuals’ confidence in following hand hygiene regulations or protocols, turned out to be relatively lower than behavioral beliefs (5.15±0.58) or normative beliefs (5.26±0.81). The results of this study appeared to be similar to those of a study conducted by Jung et al.[19], which explored hand hygiene beliefs among Korean nurses, demonstrating that similar issues do exist not only among dental workers but also among medical workers.
Questionnaire items regarding control beliefs consisted mainly of factors that obstruct hand hygiene behaviors, and limited time, troublesomeness and staff shortage were investigated and determined to be such factors through a study conducted in Korea by Kim et al.[20]. According to “2015 Year Book of the Korean Dentistry” [21], 27,086 dental hygienists were working in general hospitals, dental hospitals and clinics in 2014, while the number of outpatients per day was 650,935. Furthermore, based on reports from studies conducted on some dental hygienists in Korea, most dental hygienists in Korea perform not only typical dental hygiene tasks (80.7%) but also other tasks such as dental assisting tasks(90.3%), handling all aspects of dental care services . Therefore, the number of outpatients per a dental hygienist could be slightly greater than 24 per day[22]. As of 2014, the numbers of patients per one dental hygienist in a year with respect to different dental settings are 19,091 in dental hospitals, 215,538 in dental clinics, and 416,306 in general hospitals[21], which imply that the lack of concrete standards for appropriate numbers of patients per the number of medical personnel stated by related authorities could lead to overall shortage of time for these dental workers which in turn hinder their hand hygiene behaviors.
Although most dental care procedures are proceeded after wearing gloves, these dental workers are still expected to keep their nails short[10], and also recommended to remove manicures or “nail art” pieces within 4 days after applying them as pathogens could be accumulated in small cracks or damaged parts on nail surfaces[23], which in turn could lead to cross infections in patients during standard dental care procedures[4]. And for the same reason, repair or removal is recommended within 10 to 15 days after applying manicures or “nail art” parts[24]. Based on the results from this study, the rate of “nail art” experience over the last 2 years period was significantly higher in smaller hospitals compared to larger work settings, and significant differences were detected in terms of current “nail art” experience rate among participants with respect to their job titles and work settings (p<0.05). Participants working in dental clinics not only showed the highest scores in both types of “nail art” experiences but also scored the lowest in nail hygiene behaviors. This could be due to the fact that dental clinics are the smallest in terms of the work setting size involved in the study and therefore the work atmospheres or cultures may be relatively less restricted and more free, allowing these dental workers to behave more freely and explore their interests in “nail art” cultures[25].
Although nail hygiene behaviors show significant positive correlations with dental workers’ hand hygiene beliefs and “nail art” experiences, the correlations were not as large as expected. One of the considerable reasons for this could be that only a small number of survey questions were developed in the study for measurement of nail hygiene behaviors. While guidelines for nail hygiene of health care professionals are only included as some parts of hand hygiene guidelines, nail length, nail trimming and applying “nail art” products or manicure are not clearly outlined in resources such as CDC’s “Recommendations from the Guidelines for Infection Control in Dental Health-Care Settings”[26]. Furthermore, although WHO[10] states that health care professionals should keep their nails short and should avoid applying “nail art” products or manicure, more specific guidelines should be outlined. Also, long nails, sharp nail tips and applying decorative accessories on nails can be serious issues as they could make tiny holes or tear up gloves. More tangible and practical considerations should follow at this point among members of the field of dental hygiene in order to develop and implement guidelines such as prohibiting “nail art”[3] or maintaining appropriate nail lengths[10] into infection control education.
The hypothesis of the study that greater hand hygiene beliefs would result in better nail hygiene behaviors was supported by the results as better nail hygiene behaviors were detected with respect to higher behavioral and normative beliefs for hand hygiene and less “nail art” experiences now or over the last 2 years. Furthermore, concerns about possible infections resulting from applying “nail art” or knowledge, as well as personal style or value might have affected participants’ current choice not to apply “nail art” products or manicure or over the last 2 years period.
The purpose of this study was to determine the relationship between hand hygiene beliefs and nail hygiene behaviors, and results from the study concluded that hand hygiene beliefs affect nail hygiene behaviors. Although the completeness of the survey tool developed through this study might not be as optimal as expected, it is still meaningful that nail hygiene behaviors in dental workers were measured for the first time. Furthermore, the significance of this study also arises from the fact that it raised attention to the possible risks or detrimental problems associated with “nail art” experiences in dental workers, and therefore, aspects of nail hygiene should be more concretely incorporated into infection control guidelines for dental settings. Therefore, dental workers’ nail hygiene behavior is one of the key factors that affect infection control in dental settings. This study could function as an opportunity to promote the importance of nail hygiene maintenance and establish more practical and realistic guidelines and methods to encourage dental workers to keep their hands and nails clean at all times. But, it is necessary to revise the survey instrument for investigating dental workers’ nail hygiene behaviors developed in this study to a greater degree of completeness through further studies. Also, since the subjects of this study were limited to dental workers in only some area of Korea, it is necessary to conduct nationwide or global scale surveys.
Conclusions
The objective of this study was to analyze the relationship between hand hygiene beliefs and nail hygiene behaviors among dental workers. The subjects were 291 dental workers including dental hygienists working full-time at dental clinics, dental hospitals, general dental hospitals and dental university hospitals in Seoul, Incheon and Gyeonggi-do.
1. Scientifically significant relationships were detected in terms of participants’ clinical experiences with respect to behavioral and normative beliefs(p<0.05).
2. Participants working in general dental hospitals and dental university hospitals demonstrated the highest scores for all three of behavioral, normative and control beliefs(p<0.05).
3. Participants working in dental clinics demonstrated the greatest “nail art” experience rates in the last two years (45.5%) and at the time of the survey (15.7%)(p<0.05).
4. Nail hygiene behaviors were more likely to be observed in individuals with stronger behavior and normative beliefs (p<0.05).
Dental workers’ hand hygiene beliefs appeared to be related to nail hygiene behaviors. In particular, dental workers who have experienced some forms of “nail art” were less likely to engage in nail hygiene behaviors. In order to achieve the most optimal dental care services in terms of both patients’ and practitioners’ safety, more specific infection control guidelines for dental workers with respect to “nail art” should be established and promoted.

