Introduction
The dental arch is an interesting area of study in dentistry because of the variety in its form. This is especially important because of the basic data on the treatment plane of the tooth correction and the orthognathic surgery [1]. It has been studied about the size, position of tooth and dental arch to make a stable, functional, and aesthetic dental arch [2-4]. There are studies on the modality of malocclusion correction according to regional differences in anatomy [2], the effect of tooth size and dental arch size on the crowding [3], and comparison of arch forms between Korean and Japanese patients with malocclusion [4].
Since the 1970s, rapid development has improved diet, resulting in a change in the physique, body shape, and facial shape of individuals [5]. In a study by Kim [6], the average height of a 14-year-old was 152.0 cm in males and 151.0 cm in females in 1970, and 162.5 cm in males and 156.6 cm in females in 1990. Body weight was 43.7 kg in males and 43.8 kg in females in 1970, and 51.9 kg in males and 49.6 kg in females in 1990. According to a recent study [7], the average height and weight of Korean children and adolescents between 2006 and 2015 were 167.9 cm in males and 159.2 cm in females, and 58.4 kg and 52.8 kg in males and females, respectively. Height and weight are constantly increasing.
Angle [8] stated that teeth in normal occlusion are located on a line matching the shape and position of the arch, and Sved [9] stated that the dental arch was shaped by the function of each tooth, and the teeth were accordingly arranged on the spherical surface. The size discrepancy of the jaw and teeth can affect the dental arch and lead to teeth crowding and malocclusion [10]. Orthodontic treatment improves teeth arrangement and occlusion, but post-treatment stability is affected by the size of the dental arch [11,12].
Data on growth and changes in the dental arches are important for analyzing the physique changes with age and understanding how these changes are related to the dental arches. As the physique improves, size of the dental arches is predicted to change. Therefore, it is necessary to analyze the size of the dental arch according to the physique and use the results in the treatment plan.
Recently, various studies on the dental arch have been reported [1,4,11,13-19]. There are studies on the size of the dental arch according to malocclusion [4,13], size of the dental arch according to race [4,14], changes in the dental arch after orthognathic surgery [1,15], effects of tooth extraction on the dental arch [11,16], changes in the dental arch according to age [17,18], etc. However, studies on the size of the dental arch according to physique are insufficient. The previous study was limited to females [19]. Therefore, we aimed to measure the physique of males also and analyze the correlation between the dental arch size and physique.
Methods
1. Study subjects
The study subjects were 120 students of the C college in Suncheon city. The purpose and method of the study was explained, and they were asked to fill out the questionnaire, to which signed the informed consent. The survey period was five days, from November 26 to 30, 2018, and the questionnaires were collected directly by the researcher. Ninety-nine questionnaires were used for the final data analysis, excepting those of 17 experienced patients undergoing orthodontic treatment with tooth extraction, and those of four missing and incomplete responses. The plaster models of their dental arch were made after impression taking.
The minimum number of study samples was calculated as 84 using the G*power 3.1[20,21] program by correlation analysis with a significance level of 0.05, test power of 80%, and 0.3 effect size. Assuming the rate of elimination as 20%, 120 subjects were suitable for the analysis. The size effect was referenced from the results of the study by Han et al. [19], which analyzed the correlation between size of the dental arch and physique of the dental students.
This study was approved by the 00 Institutional Review Board (CA17-190326-HR-001-01).
2. Study method
The questionnaire consisted of eight questions, including four questions on general characteristics including weight and height, respiration, orthodontic treatment experience, tooth extraction experience, and favorite food. The items were modified and adapted according to the study purpose by referring to the survey questionnaire by Han et al. [19].
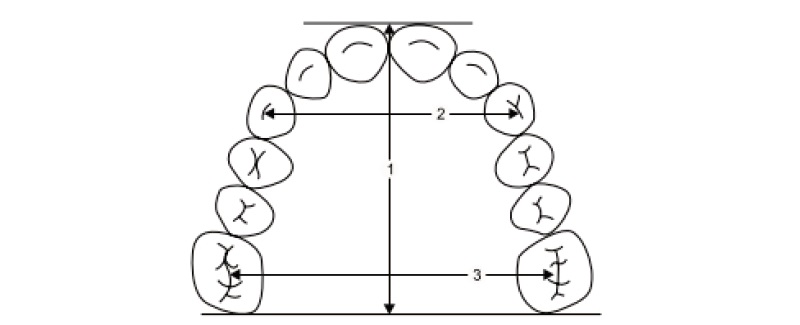
The surveyor made plaster models after recording impressions of the dental arches of the subjects with alginate impression material. The measurements are shown in <Fig. 1>. Length of the dental arch is the distance from the incisal edge of the central incisor to the distal surface of the first molar; inter-canine width is the distance between tips of cusps of the left and right canines; inter-molar width is the distance between the mesiobuccal cusps of the left and right first molars. Size of the dental arch was measured using a vernier caliper (Digimatic caliper, Sincon, China).
3. Data analysis
Independent t-test was used to compare the differences between the length and width of the dental arches according to the general characteristics. Pearson correlation coefficient was calculated for the correlation between the physique and size of the dental arch. The statistical significance level was p-value of less than 0.05. The data were analyzed using SPSS (ver. 18.0, Chicago, Illinois, USA).
Results
1. General characteristics of the study subjects
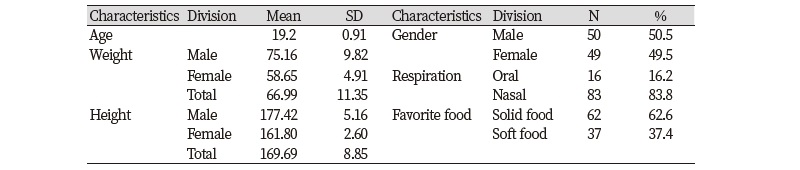
The study subjects were 99 students of the Cheongam College, and their details are shown in Table 1. Their average age was 19.2 years, and average weight and height were 66.99 kg and 169.69 cm, respectively. Of the subjects, 83.8% had a nasal breathing and 62.6% preferred solid food.
2. The length and the width of dental arches according to the general characteristics
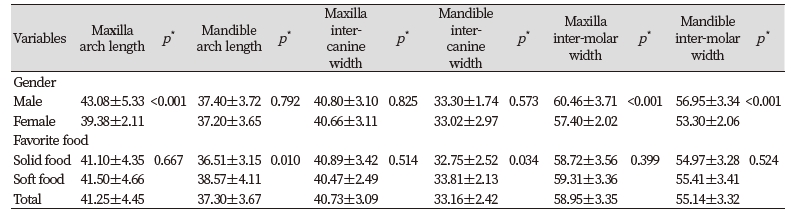
The length and width of the dental arches according to the general characteristics have been presented in Table 2. Males had 3.70 mm longer maxillary arch than females (p<0.01), 3.06 mm longer inter-molar distance (p<0.01) in the maxilla, and 3.66 mm longer inter-molar distance in the mandible (p<0.01). Other variables did not show a statistically significant difference between the sexes.
The subjects whose favorite was soft food had 2.07 mm longer mandibular arch length than the subjects whose favorite was solid food (p<0.05), and 1.06 mm longer inter-canine distance in the mandible (p<0.05). There were no statistically significant differences in other variables according to the favorite food.
3. Correlation between the physique and size of dental arch
Correlation between the physique and size of the dental arch is shown in Table 3. As height increases, the weight also increases (α=0.683, p<0.01). In addition, the maxillary arch length (α=0.373, p<0.01) and the molar width of the maxilla (α=0.214, p<0.05) and mandible (α=0.280, p<0.01) also increases. More the increase in weight, more the maxillary arch length increase (α=0.392, p<0.01). Molar width of maxilla (α=0.336, p<0.01) and mandible (α=0.502, p<0.01) also showed an increase.
Discussion
Rapid growth of the economy and improved diet have led to a significant increase in height and weight when compared to the past in Korea. As physique increases, size of the dental arch will change too. As the physique grows, the dental arches grow, and the mismatch of the maxillary and mandibular teeth causes malocclusion. Growth of the body and size of the dental arch are important because they are the basis for diagnosing and treating malocclusion.
The average age of the subjects included in the study was 19.2 years, height was 169.7 cm (male 177.4 cm, female 161.8 cm), and weight was 66.9 kg (male 75.2 kg, female 58.7 kg). In 2015, a 19-year-old Korean had an average height of 168.4 cm (male 173.4 cm, female 160.7 cm) and weight of 66.1 kg (male 71.1 kg, female 58.3 kg) [20]. In the study by Han et al. [19], females had a height of 163.2 cm and weight of 52.3 kg. The height of females in this study was lower than that in the study of 2013 and somewhat higher than the average height in Korea in 2015. The weight was also more. Although there are some differences, age is not considered a significant variable because all subjects in the study were adults.
In the mandible of females, length of the arch was 37.20 mm, inter-canine width was 33.02 mm, and distance between the molars was 53.30 mm. In the study by Han et al. [19], these were 31.8 mm, 26.8 mm, and 40.5 mm, respectively. These values are respectively 23.7 mm [21], 26.6 mm, 45.8 mm in the study by Hwang et al.[21]. The size of the arch form was more than that of the previous study [20,21]. Similar to the previous studies [20,21], the width was larger than the length. Hwang et al. [21] reported that the width of the dental arch narrowed due to changes in eating habits, and predicted that this trend will progress in future. These changes in the arch form need to be further investigated.
Variations in the size of the dental arch by sex showed greater size in males than in females. However, there was a statistically significant difference in the maxillary arch length (p<0.01) and the maxillary molar width (p<0.01). These results may be justified by the fact that physique of males is greater than that of females. Some studies have reported no differences in the size of dental arches between sexes [22-24], while others have shown that males have larger arch length [25,26]. Follow-up studies on various age groups are needed to verify the differences in the size of the dental arches by sex.
No large difference in the size of the arch according to the favorite food was found. There was a statistically significant difference in the arch length of the mandible and mandibular inter-canine width, but the difference was small. There was no statistically significant difference in the previous study [19]. Processed foods have reduced the demand for masticatory muscles and teeth. In the survey of medieval skulls, modern humans were found to have smaller depth and width of dental arches than their ancestors [27,28]. Follow-up studies are needed to determine the size of the dental arch according to the favorite food during the growing period.
As the physique increased, size of the dental arch increased. In particular, there was a statistically significant difference in the length of the arch and molar width. In the study by Han et al. [19], there was a statistically significant correlation between the weight and size of the dental arch. As the weight increased, inter-canine and inter-molar widths increased. However, there was no correlation with height. There was no correlation between height and weight in the previous study; however, in this study, weight increased as height increased.
This study has a limitation of generalization, as measurements were performed only for some college students, and the physique of males and females was not similar. However, unlike previous studies [19], the males were also measured, except those who had undergone extraction and orthodontic treatment that could affect the size of the arch. Follow-up studies will need to investigate different age groups, breathing methods, and malocclusion types. Based on the results of this study, the cause of malocclusion, form, and size of the dental arch, stability of occlusion, and oral health can be used as basic data.
Conclusions
In this thesis, we analyzed the correlation between college students' physique and dental arch size. Ninety-nine subjects completed the questionnaire and underwent impression taking. The t-test and correlation analysis were used for analysis.
The measurements and analysis results are as follows.
1. In males, the maxillary arch length (p<0.01) and inter-molar width of the maxilla and mandible (p<0.01) were higher than that of females.
2. Differences in the dental arch size according to favorite food was not significant.
3. As height increased, the maxillary arch length increased (α=0.373, p<0.01), and molar width of the maxilla (α=0.214, p<0.05) and the mandible (α=0.280, p<0.01) also increased.
4. More the weight increase, more the increase in maxillary arch length (α=0.392, p<0.01) and molar width of the maxilla (α=0.336, p<0.01) and mandible (α=0.502, p<0.01).
The size of the dental arch in males is larger than that in females. As the physique increases, maxillary length and molar width increases. These results can be used as basic data to study the cause of malocclusion, form, and size of the dental arches, stability of occlusion, and oral health.

