Introduction
Deciduous teeth are important for chewing and pronunciation in children. They maintain the position for eruption of permanent teeth and help normal development of the jawbone. Early childhood caries (ECC) occurring in children under 5 years of age frequently occurs in maxillary primary incisors and primary first molars. Dental caries also increases according to the order of tooth eruption [1]. Therefore, even for deciduous teeth may need to be filled to reduce the risk of loss. Childhood caries can also impede the development of permanent teeth. Early loss of primary teeth due to caries can cause malocclusion by adversely affecting eruption of permanent teeth and growth of the maxilla. ECC also causes severe pain and infection. When it is associated with eating and sleep disturbances, ECC can negatively affect children’s ability to focus on learning [2]. Therefore, thorough oral health care is required to prevent dental caries from eruption of primary teeth until they are replaced with permanent teeth. According to the Statistical Information Report on the Children’s Oral Health Survey announced by the Ministry of Health and Welfare in 2019, the proportion of 5-year-olds who experienced deciduous teeth caries was as high as 68.5% and the average caries experience index per person was 3.43. This means that most children experience dental caries before complete eruption of their primary teeth (https://www.narastat.kr/metasvc/index.do?confmNo=117051&inputYear=2018, Statistical Information Report for Users_Children’s Oral Health Survey_2019.pdf). The preventive oral health care effect of dental caries is significantly higher in children than in adults because primary caries affects permanent dental caries [3].
Changes in family structure and an increase of working women have increased the demand for childcare facilities and early childhood education institutions. As the time spent in childcare facilities increases, the awareness and behavior of educators about oral care for young children have a great impact on children’s oral health. Therefore, the duty and responsibility to guide children’s oral health are being emphasized not only by family members, but also by teachers of childcare facilities and early childhood education institutions. Teachers with correct knowledge of dental practice had a lower average number of cavities in their infants than teachers without knowledge [4]. In addition, the average number of dental caries in infants was lower when childcare facilities and teachers provided correct oral care for infants. As a result of surveying the perception of oral health among preschool teachers in Seoul, 99.1% of respondents recognized the importance of oral healthcare for children. They also recognized their responsibility for providing children’s brushing instruction and oral examinations [5]. Since childcare teachers’ awareness and performance of children’s oral health closely affect children’s oral health, the need to develop an oral health education program for early childhood teachers was suggested.
To prevent the spread of COVID-19 through respiratory droplets transmission, from Feb. 29, 2020 until recently, a state-led quarantine system such as observing personal hygiene and social distancing has been maintained for a long time. Response guidelines for preventing infectious diseases were distributed to public and multi-purpose facilities. The Office of Education also distributed additional guidelines for preventing infectious diseases for kindergartens and daycare centers. Accordingly, over the past three years, kindergartens and daycare centers have been operating programs centered on individual play rather than group play while observing social distancing. In addition, for personal quarantine, continuous wearing of a mask is maintained except for eating and drinking. Various phenomena that have recently changed due to group quarantine have been reported, such as current state of the response system of daycare centers during the COVID-19 [6], the perception of kindergarten teachers on online non-face-to-face classes [7], and the phenomenological study of behavior changes in children after wearing masks in kindergarten [7]. The present study investigated changes in oral health care practices for children in kindergartens and daycare centers due to the COVID-19, trying to derive points that cause problems for children’s oral health. Through this study, we intend to present a basis for establishing children oral care policies of childcare institutions in the future.
Methods
1. Subjects and data collection
This study conducted a survey of childcare teacher working in kindergartens and daycare centers from December 13, 2021 to Jan. 2, 2022 for about 3 weeks. This is COVID-19 special quarantine period corresponding to the level 3 and level 4 social distancing guideline in Korea. The period before Mar. 2020 was set as ‘before COVID-19’. Through online community platform of childcare teachers, URL links and QR codes were provided. The survey was designed to be answered only by the teachers in charge of 3 to 5 years of age. After being provided the purpose of the study, only subjects who voluntarily agreed to the questionnaire participated in the study by checking the online consent question. A total of 193 questionnaires were returned and 189 questionnaires with responses to all questions were used as validated data, excluding 4 insincere responses.
The sample size was calculated using G*power sampling software (ver. 3.1.9.7 for Windows). The minimum required sample size was estimated to be 158 persons with an α error of 5%, power of 90%, degree of freedom of 3 and medium effect size of 0.3 by applying the chi-squared test as the main analysis method. Additional samples were collected in each group to compensate for processing errors.
Questionnaire contents used in two previous studies were partially modified and reflected to suit this study [9,10]. The questionnaire consisted of 32-item including general characteristics, oral hygiene practice, and oral education experience of children before and during COVID-19, teachers’ oral education necessity, and teachers’ oral health knowledge quiz related to childcare, dental caries, and fluoride application. The present study was approved by the Institutional Review Board of Eulji University (approval no. EU21-86).
2. Statistical analysis
The collected data were analyzed using SPSS Statistics program (ver. 28.0.1.1; IBM Corp., Armonk, NY, USA). All statistics were expressed as frequencies and percentages for categorical variables, and the chi-squared test was used to determine the statistical significance of associations between the variables. A p≤0.05 was considered statistically significant.
Results
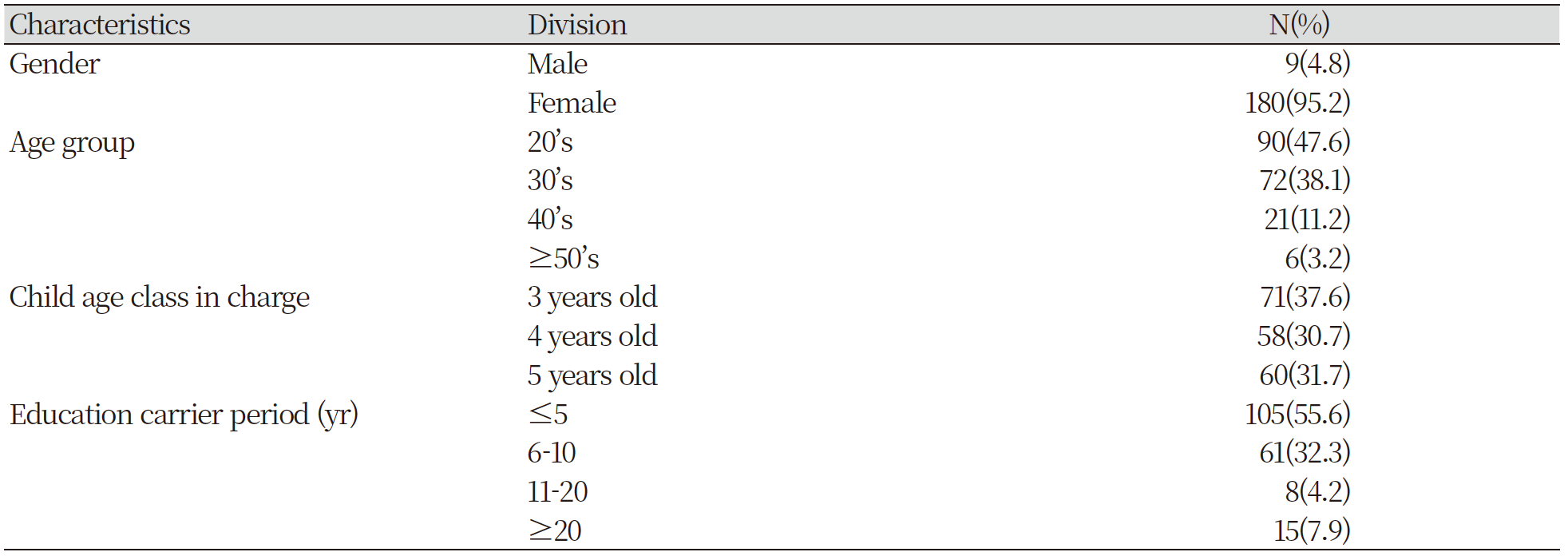
Responses of 189 kindergarten and daycare center educator were analyzed for this study. Female educators accounted for 95.2% of respondents. Regarding ages of teachers, there were 90 in their 20s (47.6%), 72 in their 30s (38.1%), 21 in their 40s (11.2%), and 6 in their 50s (3.2%). As for the positions, there were 179 (94.7%) teachers and 10 (5.3%) directors. Regarding the length of their education career, there were 105 (55.6%) educators with less than 5 years of education carrier, 61 (32.3%) with 6-10 years of education career, 8 (4.2%) with 11-20 years of education career, and 15 (7.9%) with more than 20 years of education career. Regarding the age of the children that they were in charge of, there were 71 (37.6%) children aged 3 years, 58 (30.7%) children aged 4 years, and 60 (31.7%) children aged 5 years <Table 1>.
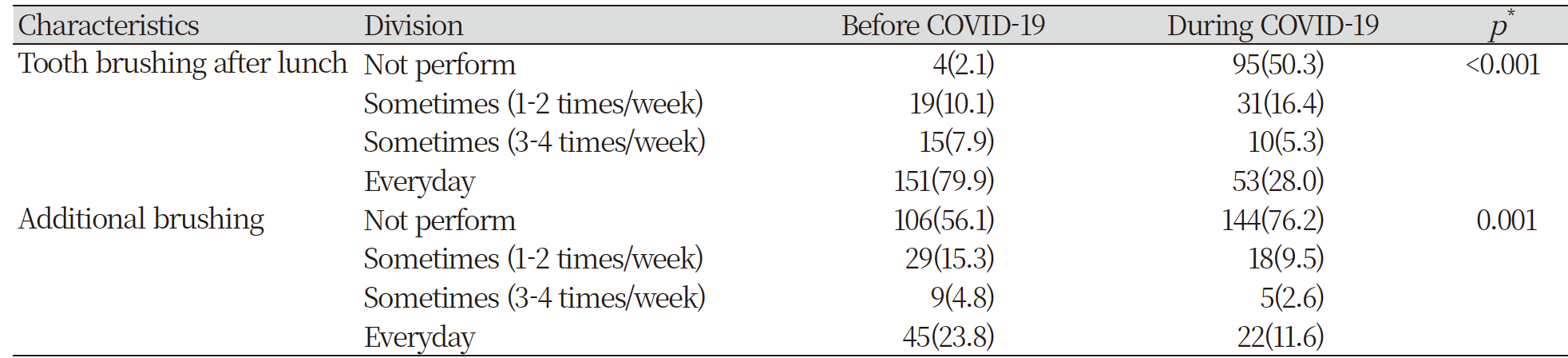
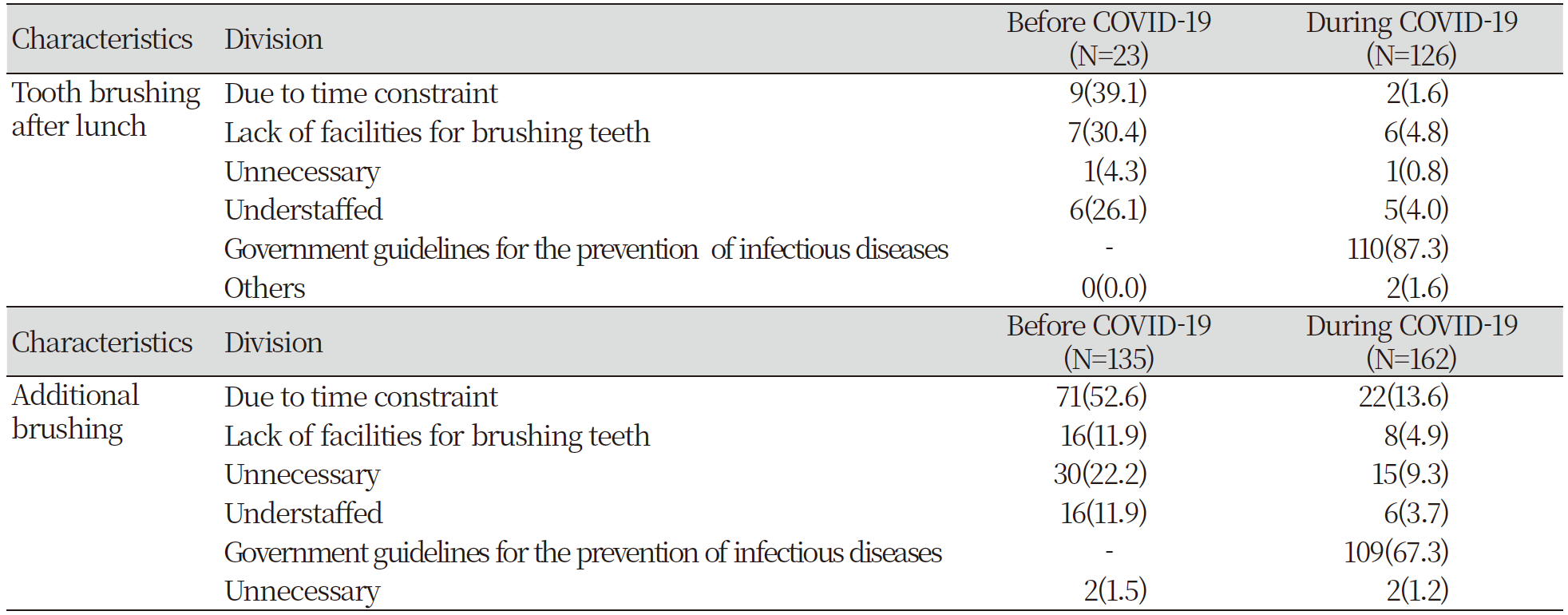
Changes in the frequency of tooth brushing before and during the COVID-19 were investigated <Table 2>. Before the COVID-19 pandemic, 79.9% of children brushed their teeth daily after lunch. However, during the COVID-19, only 28% brushed their teeth daily (51.9% decrease) with statistically significant decrease (p<0.001). On the other hand, the rate of not brushing their teeth during COVID-19 increased by 48.2%. The reason for the difficulty of brushing their teeth among respondents of ‘not perform’ and ‘1 or 2 times a week’ was lack of time before the COVID-19 pandemic [9(39.1%), n=23]. However, during the COVID-19 pandemic, it was mostly due to the government’s guidelines for COVID-19 prevention [110(87.3%), n=126] <Table 3>. The frequency of additional brushing of teeth other than brushing teeth after lunch before and during COVID-19 was also investigated <Table 2>. Before the COVID-19, 43.9% said they brushed teeth additionally occasionally or daily. However, during COVID-19, this percentage decreased to 23.8%. Additional toothbrushing frequency during COVID-19 was also significantly reduced than that before COVID-19 because of the government’s guidelines for COVID-19 prevention [109(67.3%)] <Table 3>. This result meant that oral hygiene care of infant and children in kindergarten and daycare centers was neglected during the quarantine period.
Changes in the toothbrushing instruction method between before and during COVID-19 were also investigated <Table 4>. Before COVID-19, 60% of children brush their teeth and then got checked by their teacher. This percentage decreased to 50.8% during COVID-19, although the number of children who brush their teeth was increased by 10.6% during COVID-19. The frequency of oral health education for infants and children was 88.4% before COVID-19. It decreased to 75.1% during COVID-19 <Table 5 >. The results were statistically significant (p=0.001). The frequency of oral examination was 68.3% before COVID-19. It decreased to 58.2% during COVID-19 with statistical significance (p=0.043). This result means that oral education and oral examination of infants and children have decreased since group meetings and face-to-face meetings are limited to prevent COVID-19 infection. The frequency of oral health education experience for childcare teachers also decreased by 8.5% due to COVID-19. On the other hand, the demand for oral health education of childcare teachers during COVID-19 was very high at 95.2% <Table 6 >. Of 180 childcare teachers who requested oral health education, the highest ‘desirable oral health educator’ was an oral health officer in public health center (52.8%), followed by a dentist (27.8%) and a dental hygienist (16.1%) <Table 7 >.



|
Table 7. Desirable oral health educator for childcare teachers (N=90) 
|
|
All values are presented as N(%) for categorical variables. |
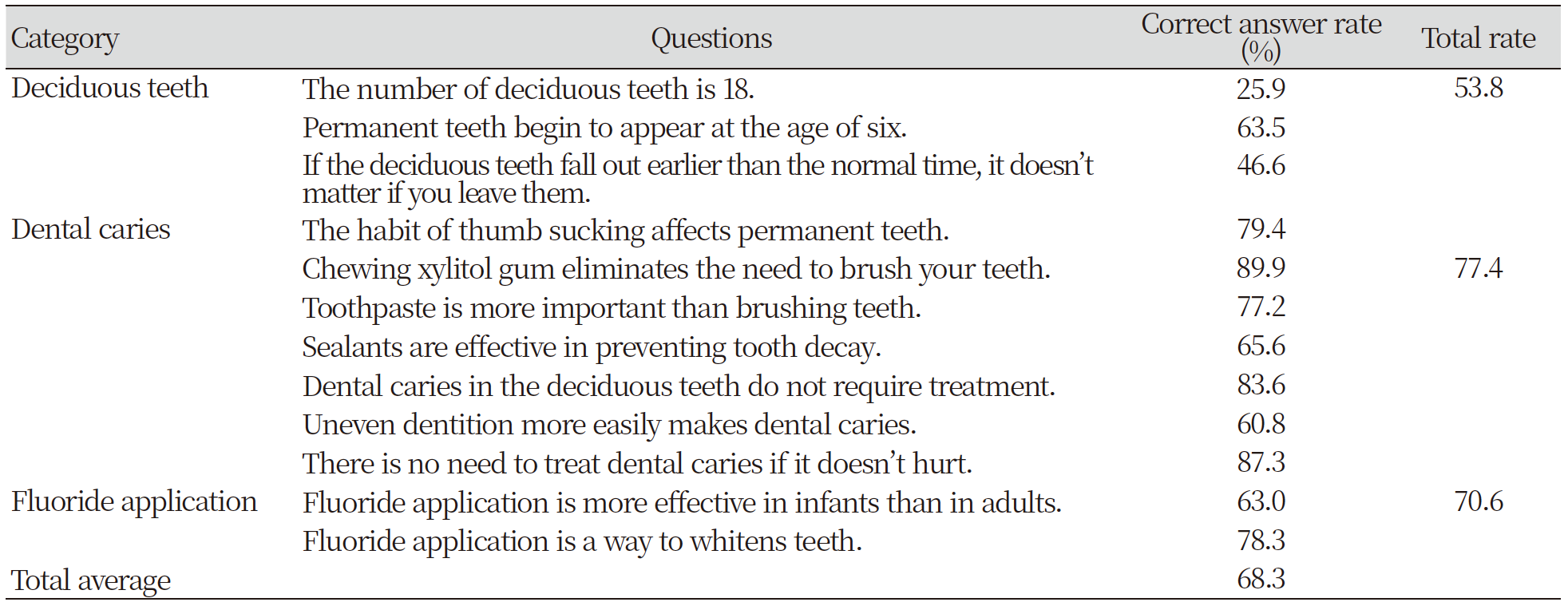
Deciduous teeth, dental caries, and fluoride application related issues were tested to determine oral health knowledge levels of childcare teachers. There were 8.2 correct answers to 12 questions, representing an average of 68% <Table 8 >. The correct answer for dental caries-related question was an average of 76% and the correct answer for fluoride application-related question was an average of 77%. On the other hand, correct answer for deciduous teeth related question had an average of 55%. Among items related to deciduous teeth, the correct answer to the effect of thumb sucking on deciduous teeth was high (79.4%), whereas correct answers to the timing and maintenance of eruption of deciduous teeth (46.6%) and the number of deciduous teeth (25.9%) were the lowest.
Discussion
The main goal of this study was to examine the changes in oral health care for children before and during COVID-19 in kindergartens and daycare centers. We found that the oral health care of children, including tooth brushing, oral examinations, and oral health education, in kindergartens and daycare centers has significantly declined during COVID-19.
According to the Korean Children’s Oral Health Survey conducted every three years according to the Oral Health Act, the rate of experiencing dental caries among 5-year-olds is as high as 68.5%, suggesting that most children experience tooth decay before their primary teeth erupt completely (https://www.narastat.kr/metasvc/index.do?confmNo=117051&inputYear=2018, Statistical Information Report for Users_Children’s Oral Health Survey_2019.pdf). As social distancing to block the spread of COVID-19 and the obligation to wear a personal mask are maintained for a long time, factors that can harm oral health might have accumulated due to limited oral hygiene management in kindergartens and daycare centers that educate young children. Therefore, in this study, we investigated the status of oral health care for children before and during COVID-19 through a questionnaire targeting kindergarten and daycare center teachers and identified factors that could hinder promotion and maintenance of children’s oral health.
Early childhood education institutions provide snacks and drinks in addition to lunch [5]. Fruit is served most frequently, followed by bread, vegetables and cereals. Milk is the most frequently served drink, followed by yogurt and fruit drinks. These are highly carbohydrate-containing products that are highly associated with dental caries. In this study, changes in brushing performance after lunch as well as after snack were investigated before and during COVID-19. As a result of the survey, the percentage of kindergartens and daycare centers that did not ask children to brush their teeth after eating increased from 2.1% to 50.3% during the COVID-19 pandemic. The percentage of institutions that do not ask children to perform additional brushing other than after meals also increased from 56.1% to 76.2% during the COVID-19 pandemic <Table 2>. Tooth brushing practice was dramatically reduced to prevention of droplet infections. Even in a report surveyed in 2020, the early days of the COVID-19 issue, the proportion of kindergartens and daycare centers that did not brush their teeth after meals increased significantly during the COVID-19 period, and the proportion of institutions that did not brush their teeth other than brushing after lunch also increased during the COVID-19 period [5]. In addition, during COVID-19, teacher’s inspection of children’s oral condition after teeth brushing decreased from 60% to 50.8% <Table 4>. This means that oral hygiene management for children who have to stay for a long time in the institution is becoming poorer. The Korean Children’s Oral Health Survey will be conducted in the next cycle. It will produce results reflecting the impact of COVID-19. It is predicted that oral hygiene practices that are continuously restricted under the influence of COVID-19 regulations will be harmful to the oral health of infants and children. Regular oral health education and oral examinations for infants and children have also been reduced by about 10-12% since COVID-19<Table 5>. Due to social distancing caused by the COVID-19 epidemic, oral care for children at kindergarten and daycare centers was insufficient. Children who received oral examinations had more dental clinic visits. However, the cost of dental treatment was higher for children who did not receive oral examinations [11]. A decrease in the number of oral hygiene and oral examinations can cause not only harm to the oral health of growing children, but also can increase oral treatment costs in the future. Thus, prompt improvement is required. In a study comparing the oral hygiene behavior of pre-schoolers in Wuhan city during the sudden outbreak of COVID-19 with pre-schoolers residing in non-Wuhan, Wuhan children brushed their teeth more actively [13]. However, even if infectious diseases are adequately defended in the future, the intention of direct dental visits of Wuhan residents was lower than that of non-residents. These results suggest that the experience of being affected by a severe infectious disease may have long-term implications for future dental visits. Therefore, considering the long-term experience of infectious diseases, it is also necessary to provide the importance of oral healthcare through continuous counseling so that dental care is not restricted due to concerns about future infection.
Oral health education experience of childcare teachers has a significant impact on oral health education and practice for children. Thus, regular oral health education was necessary [10]. Childcare teachers in kindergarten and daycare centers recognize the importance of deciduous teeth and the necessity of brushing their teeth. They also recognize the need for oral education and oral examination. They acquire oral health knowledge mainly through online information, TV, and dentistry [14]. According to our survey results, the experience of oral health education of childcare teachers during COVID-19 decreased from 76.2% to 67.7%, although the demand for oral health education was very high at 95.2% <Table 6>.
In order to find out oral health knowledge of childcare teachers, a total of 12 questions related to deciduous teeth, dental caries, and fluoride application were used. The percentage of correct answers was 8.2 (68.3%) out of 12. Percentages of correct answers to questions related to deciduous teeth, dental caries, and fluoride application were 53.8, 77.4%, and 70.6%, respectively. Knowledge related to deciduous teeth was the least. In particular, there was a lack of knowledge about the number of deciduous teeth (percentage of correct answer: 25.9%) and problem of early loss of deciduous teeth (percentage of correct answer: 46.6%). Also, knowledge about the relationship between malocclusion and dental caries (percentage of correct answer: 65.6%), the relationship between dental caries and sealants (percentage of correct answer: 60.8%), and the effect of fluoride application to infants (percentage of correct answer: 63.0%) were relatively low <Table 8>. Therefore, oral health education for childcare teachers is required to include information related to them. In particular, the awareness level of the dental caries prevention effect of childcare teachers was significantly higher among those with more than 10 years of educational experience [15]. According to the 2021 basic statistics on education (https://www.moe.go.kr/boardCnts/view.do?boardID=294&boardSeq=88238&lev=0&searchType=null&statusYN=W&page=1&s=moe&m=020402&opType=N), the average age of kindergarten teachers registered with the Ministry of Education is 34.8 years old. Since the average age of daycare teachers managed by the Ministry of Health and Welfare is not reflected, the average age of daycare center and kindergarten teachers may be different. The age of daycare center and kindergarten teachers who participated in this study was 47.6% in their twenties. In addition, 55.6% of the participants had less than 5 years of educational experience. Therefore, considering age and education carrier period, it is necessary to provide an education program for improving oral health knowledge to prevent dental caries in children for a significant proportion of childcare teachers. In addition, in order to recover the lack of oral hygiene management for child that has persisted for the past 3 years, oral hygiene behaviors for children should be implemented through active oral health education for childcare teachers.
According to a previous report, professional personnel of dental hospitals are suitable for infant oral health education [14]. On the other hand, oral health officer in public health center (52.8%) was found to be the most suitable for oral health education for childcare teachers, followed by dentistry (27.8%) and dental hygienist (16.1%) in this study<Table 7>. Before COVID-19, regular oral examinations at kindergartens and daycare centers were conducted mainly by professional personnel from dental clinics. The prolonged social distancing has caused a change in the perception of oral health educators. In particular, the suitability of dental hygienists as oral health educators as well as dentists was relatively low. Efforts are needed to improve the awareness of dental hygienists as oral health experts. Considering our results and the current public health care system in Korea, oral education by dental hygienists should be enhanced in the way of community oral health programs through cooperation with local dental hospitals. Active oral health activities through participation in education of dental hygienists for childcare teachers and community service are required.
Some limitations of our study should be noted. We did not consider area variables that may affect similarities and differences in oral health behaviors including affiliated institutions in the COVID-19 pandemic. In addition, this study did not overcome the issue of analytical biases by asking questions about the before COVID-19 situation, that is, recall bias.
However, this study has several strengths: (1) this is timely study providing the changes in oral health care for children before and during COVID-19 and (2) our study provided reliable information and results due to the Intensive survey period with same level of COVID-19 quarantine which affected people’s behavioral patterns according to government’s quarantine guidelines and social distancing levels
In this study, we confirmed that oral hygiene management for children was insufficient due to COVID-19. Efforts to recover it are urgently needed. Efforts should be made for oral hygiene management of children through close communication between childcare institutions and caregivers. In addition, continuous activities are needed to raise awareness of dental hygienists as suitable oral health care educators.
Conclusions
To investigate the changes in oral health care for children before and during COVID-19 and the perception of oral health care, a total of 189 teachers of kindergartens and daycare centers were analyzed.
1. Oral health care of children, including tooth brushing, oral examinations, and oral health education, has significantly declined during COVID-19.
2. Educators in kindergarten and daycare center responded that an oral health officer at a public health center was the most desirable oral health educator.
The oral health care behavior among children and teacher in kindergarten and day care center was significantly influenced by the COVID-19 epidemic, which might give rise to a long-term impact on oral healthcare in the future. The findings suggested that more attention to children as well as teacher among kindergarten and daycare center might be needed in order to maintain oral health.

