Introduction
Quality of Life (QOL) refers to health care in a wider area than health promotion. It is the sense of satisfaction and happiness that affect complex factors such as subjective physical health, self-reliance, social relationships and environment, and psychological condition [1].
As oral health is closely related to physical health, it also affects subjective satisfaction and happiness [2]. Oral health, which is essential to maintain the quality of life, refers to not only the condition affected by it, but also the healthy maintenance of the teeth and maxillofacial oral structures to maintain a psychologically and socially comfortable life. In the present day health management, the scope has been expanded from the disease-centered approach to the socio-psychological multi-factor approach [3]. Also, the development of measurement instruments has been attempted as a part of a psychosocial approach based on the individual experiences in the regional community environment, in addition to the traditional clinical measurement methods, through studies that have suggested that it is possible to evaluate oral health-related quality of life by measuring the oral health-related needs. The method to measure these needs is the Oral Health-related Quality of Life (OHRQoL), and this can evaluate a particular oral health condition [4].
Oral health impact profile (OHIP), which is one of the instruments that measure OHRQoL, is based on the Locker’s conceptual model of oral health [5]. It is an instrument on the effect of oral disease on the society, comprised of a total of 49 items across 7 domains of Functional Limitations, Physical Pain, Psychological Discomfort, Physical Disability, Psychological Disability, Social Disability and Social Handicap. Currently, it has been reduced to 14 items and tested for reliability and validity as the OHIP-14 and is being used to assess OHRQoL [4]. OHIP can be efficiently used to evaluate the clinical diagnosis and self-perception of oral health. It can provide another direction in the oral health management research [6]. A debate on the consistency of OHIP across cultures has been started, thus implying its importance [7-9]. Due to these developments, OHIP-49 has been used in various studies of infectious diseases on the middle-age and elderly people in Australia, United States, and Canada [8,10]. The reliability and validity of OHIP-49 and OHIP-14 were also confirmed in geriatric research in Korea [11], and many studies have been conducted to identify related determinants [12-28]. Most studies measuring oral health-related quality of life in Korean elderly used OHIP-14 and reported various factors affecting oral health-related quality of life.
Therefore, the purpose of this study is to identify major factors that determine the OHRQoL of the elderly through a systematic review.
Text
1. Study design
This study is a literature review to systematically identify the major determinants from the quantitative results of individual studies on the OHRQoL of the Korean elderly.
2. Data search and selection
1) Search strategy
Publications about the OHRQoL of the Korean elderly were selected. A literature search was carried out on Korean journals published up to January 10, 2019, using electronic databases.
The databases used for the search were RISS, KISS, eArticle, and DBpia. The keywords used for the search were “elderly,” “OHRQoL,” “oral,” and “quality of life.” For final data selection, two researchers independently reviewed the literature searched through the electronic database using endnote and agreed to determine whether to include each study in the final selection.
2) Data selection and review strategy
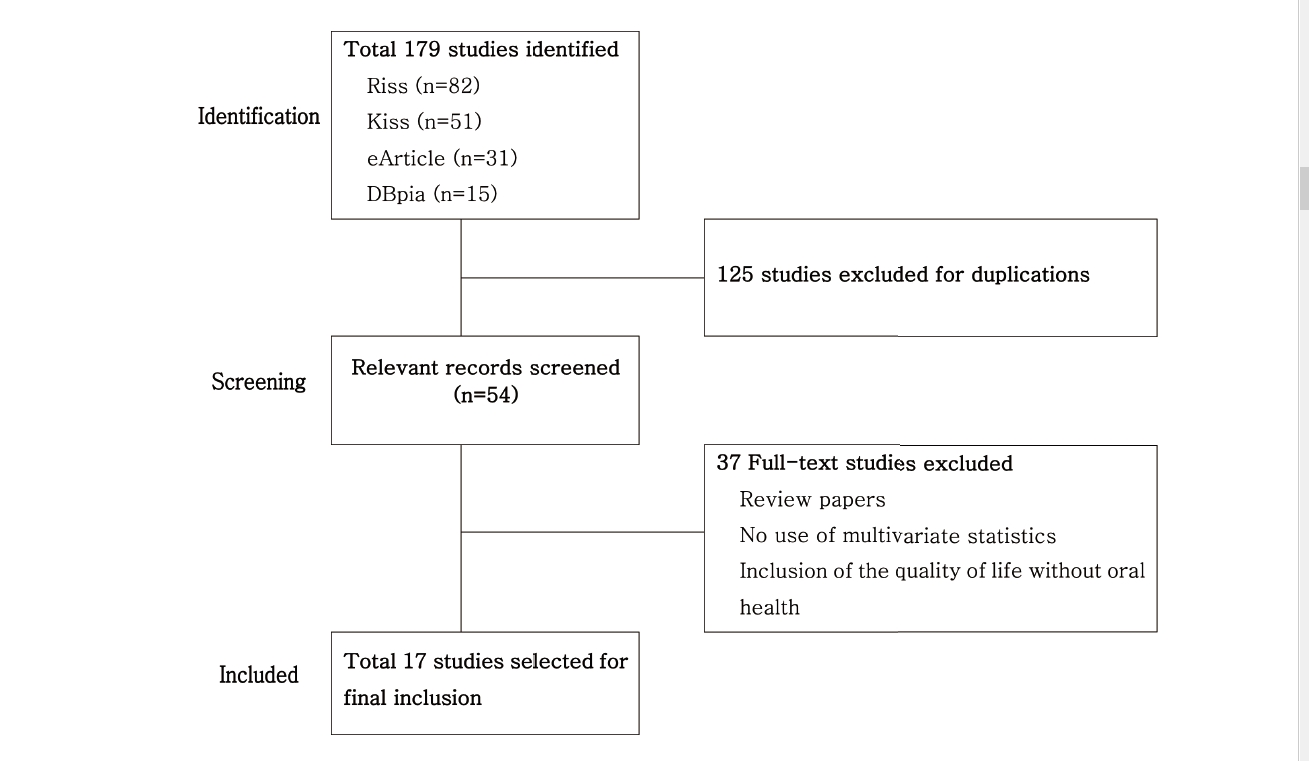
Figure 1 shows the process of the final literature review. A total of 179 publications were identified as a result of the literature search. A total of 82 publications were found on Research Information Sharing Service (RISS), 51 were found on Korean studies Information Service System (KISS), 31 were found on eArticle, and 15 were found on DBpia. From a total of 179 publications, 125 duplicates were excluded by checking the title, authors, year of publication, and journal of publication. The 54 were reviewed after excluding 125 with a focus on the research title and abstract. A total of 37 studies that used OHRQoL as the outcome variable but did not analyze the relationship or were on quality of life that is unrelated to oral health were excluded. Furthermore, cases that were difficult to determine from the abstract alone were reviewed in whole to make the final selection of literature. Finally, a total of 17 publications met the conditions.
3. Data analysis
The 17 studies used for data analysis were coded according to their year of publication, sample size, sex, and statistical analysis methods for the sub-group analysis on the major categorical variables. After categorizing the factors, the related factors of the group and effect sizes were coded. For effect size, the sign, value, and correlation effect size were coded. The coding was performed by the researchers and one research assistant. One advising professor of dental hygiene major reviewed the coding and the categorization of sub-variable groups. The researchers reviewed the coding after it has been coded. After the review, abnormalities, and parts that need confirmation were checked and corrected. Items that were inconsistent after the review by the researchers were revised and supplemented.
4. Results and Discussion
1) General characteristics
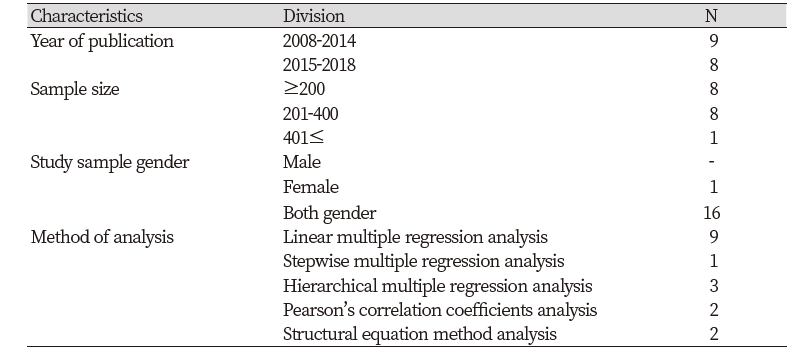
The year of publication of the study on the OHRQoL of the elderly was between 2008 and 2014 for 9 studies, and between 2015 and 2018 for 8 studies. The sample size was 200 or below for 8 studies, between 201 and 400 for 8 studies, and 401 or more for one study. For sex, 16 studies were on both male and female subjects and one study was on only female subjects. The data analysis method was most commonly multiple regression analysis for 9 studies, or stratified regression analysis for 3 studies or stepwise regression analysis for one study. Although there were many studies conducted using a correlational analysis along with the regression analysis, there were 2 studies that used only correlational analysis and 2 that used structural equation method <Table 1>.
2) Determinants of the OHRQoL of the elderly
This study examined the determinants used in previous Korean studies related to the OHRQoL through a systematic review. The results of previous Korean and international research use different variables for each researcher, and report by applying various measurement instruments and research methods. Thus, there are difficulties in drawing integrated conclusions about the determinants of OHRQoL. Furthermore, there are protective factors that have a positive correlation with OHRQoL and risk factors that have a negative correlation with OHRQoL. Thus, the factors of each study varied not only in direction, but also in size.
Table 2 categorized the significant variables that affect the OHRQoL of the elderly and instruments used to measure it. In addition, if there were more than 20 statistically significant variables among the correlation variables, the categorizations were made based on the variables with a strong correlation.
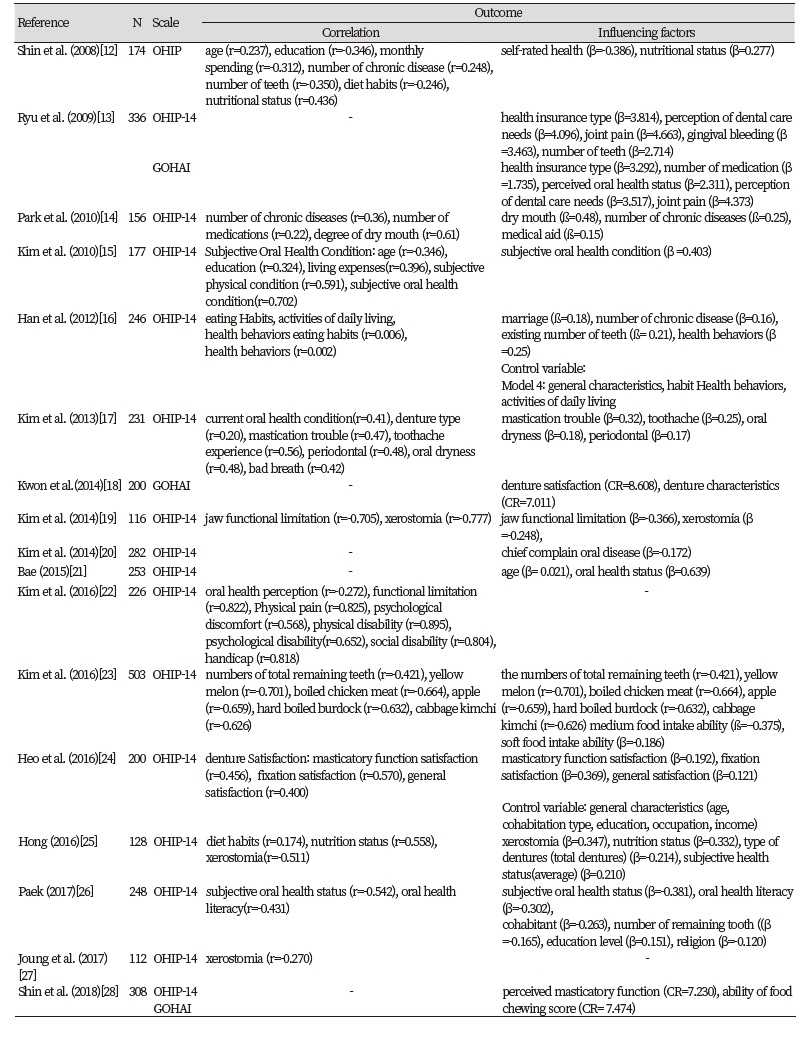
Among the total of 17 studies, 16 measured OHRQoL using Oral Health Impact profile-14 (OHIP-14). Among those 16, 2 studies [13,28] used OHIP and Geriatric oral health assessment index (GOHAI) simultaneously, while one study only used GOHAI [18]. The results of categorizing the determinants of the OHRQoL of the elderly by common characteristics showed that 4 studies related to food and diet [12,16,23,25], 5 studies related to xerostomia [14,17,19,25,27], and 4 studies on denture satisfaction and characteristic’s related to dentures [18,20,24,25]. The remaining studies used variables related to the subjective oral condition and oral health perception.
It was found that most research variables were used in many studies without being categorized by particular criteria. Among food and diet-related variables, nutritional status, moderate food intake ability, and soft food intake ability affected OHRQoL. Additionally, xerostomia, number of diseases, and medication affected OHRQoL. Factors such as age, denture satisfaction, marital status, oral condition, type of health insurance, health behavior, number of remaining teeth, mastication ability, and oral health literacy were found to affect the OHRQoL of the elderly.
This study limited the scope to examine the correlation coefficients and regression coefficients from correlation and regression analyses, from which the factors that affect OHRQoL can be identified. There were limitations in identifying the effect size, because most of the individual studies that were analyzed were conducted using a cross-sectional design and there was no experimental or interventional research to enhance the OHRQoL of the elderly.
To summarize the main results of the analysis, most of the factors related to the OHRQoL of the elderly were diet-related variables [12,16,23,25]. Other factors were xerostomia [14,17,19,25,27], denture satisfaction, and denture-related characteristics [18,20,24,25]. Variables used in most studies varied depending on the characteristics of the research. The factors that most strongly affected the OHRQoL of the elderly were found to be nutritional status and mastication ability. Furthermore, xerostomia, a number of physical diseases, and medication also affected OHRQoL. Age, denture satisfaction, marital status, oral condition, type of health insurance, health behavior, number of remaining teeth, mastication ability, and oral health literacy were found to be determinants.
Research methods to draw integrated results from individual studies that report different results include a meta-analysis [29]. Meta-analysis determines not only the conclusion about the direction but also the size of the relationship between variables, thus enabling the drawing of actual results based on evidence. Moreover, a meta-analysis has a post-hoc nature after the completion of individual studies. Thus, meta-analysis can suggest the studies that are needed and the future direction of research, rather than providing a definitive conclusion about a relationship [29].
Combined, meta-analysis research that analyzes the correlation coefficients and effect sizes is necessary to integrate the results of previous studies about the OHRQoL of the elderly that have been conducted in various research. This study was limited in that it was conducted as a systematic analysis because the validity of the results of the individual studies selected for this research could not be guaranteed due to the publication errors that prevented a meta-analysis. A future study must identify the direction and size of the relationships between the determinants through a meta-analysis of a selection of studies that have been expanded to include individual Korean and international studies about the OHRQoL of the elderly, in accordance with the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Moreover, this can contribute to improving the OHRQoL of the elderly by drawing the research theme and directions necessary to solve the current problems with the oral health of the elderly. Most importantly, research that analyzes the intervention effect through longitudinal research or interventional research must precede to find out the determinant that affects the OHRQoL of the elderly in the field of dental hygiene. It is suggested that resolutions to solve current problems will be found through a meta-analysis that draws integrated results from these individual studies.
Conclusions
The results of the major factors that determine the OHRQoL of the elderly through a systematic review of studies related to the OHRQoL of the elderly are as follows.
1. In Korea, the numbers of publications on the OHRQoL of the elderly were 9 published between 2008 and 2014, and 8 between 2015 and 2018. The sample size was 200 or below for 8 studies, between 201 and 400 for 8 studies, and 401 or more for one study. For sex, 16 studies were on both male and female subjects and one study was on only female subjects. The data analysis method was most commonly multiple regression analysis for 9 studies or stratified regression analysis for 3 studies or stepwise regression analysis for one study. Although many studies were conducted using a correlational analysis along with the regression analysis, there were 2 studies that used only correlational analysis, and 2 studies used structural equation.
2. The results of categorizing the determinants of the OHRQoL of the elderly by common characteristics showed that there were 4 studies related to food and diet, 5 studies related to xerostomia, and 4 studies on denture satisfaction and characteristic’s related to dentures. Nutritional status, moderate food intake ability, soft food intake ability, xerostomia and the number of diseases, medication, age, denture satisfaction, marital status, oral condition, type of health insurance, health behavior, number of remaining teeth, masticationability, and oral health literacy were found to be the determinant of the OHRQoL of the elderly.
As shown above, various determinants of the OHRQoL of the elderly were found. Therefore, it is necessary to develop and manage the elderly oral health enhancement program that considers the factors related to the OHRQoL.

