Introduction
Stress is a psychological reaction, like anxiety or threat that a person feels when faced with a physically or mentally difficult situation [1]. It can also cause symptoms such as headaches and fatigue, and negatively affect the physical, mental and social condition of an individual, as well as their quality of life [2]. Stress can occur at any time throughout human life and has a slow rate of recovery, especially in the elderly [3]. The main causes of stress in the elderly include illness and financial loss [4]. Since elderly people lacks the ability to cope with stress, they are greatly impacted by it. In addition, it had been reported that the worse the health status, higher is the stress level [5]. Unexpected changes such as difficult economic conditions, loss of physical and mental function, and loss of their roles, are the common causes of stress in the elderly [6]. Physical aging and vulnerability to disease work as a stress for older people [7].
Functional disorders that affect oral functions including food intake, pronunciation, and aesthetics can adversely affect overall life [8]. In terms of oral health, stress is associated with dental caries, periodontal disease, and dry mouth [9,10]. The subjective oral health was reported to be poor in cases with high levels of stress [3]. Goyal et al. [11] reported that stress induced Cortisol release has a significant effect on periodontal disease and Akhter et al. [12] also reported that stress can be a potential risk factor for periodontal disease. Periodontal disease is a chief factor of tooth loss, which affects the chewing ability. In addition, an active masticatory ability can help reduce pain and stress [13]. Stress is also a potentially important factor in temporomandibular joint disorder (TMD) [14]. Hwang et al. [15] reported an association between stress and chewing discomfort, while Jung et al. [16] reported no relationship between the total number of tooth loss and perceived stress. Choi and Cho [3] also confirmed the relationship between stress and oral health.
However, few studies have previously examined an association between stress and chewing function in older adults [17,18]. Therefore, this study aimed to investigate whether stress in older adults affects number of residual teeth and chewing function using the Korea National Health and Nutrition Examination Survey (KNHANES) VI data that can represent the elderly people.
Methods
1. Study participants
This study was conducted using health questionnaires and the oral examination raw data downloaded raw data from the 2nd and 3rd year (2014-2015) of the 6th Korea National Health and Nutrition Examination Survey. Among the KNHANES VI data, data from the 2nd and 3rd year (2014-2015) with the same variable were investigated. Data were analyzed by creating a plan file with weights. The subjects were aged 65 or older. Of the 3,134 subjects, 2,002 were selected as the final subjects, excluding those who did not participate in the survey or oral examination. This study was approved by Institutional Review Board of the 00 University (KNU - 2019 - 0121).
2. Socio-demographic and stress level
The general variables included gender, age, economic activity, residence type, home income, and education level. The health-related variables included drinking, smoking, hypertension, and diabetes. Stress perception was assessed on a four-point Likert scale. 1 point is ‘very much’, 2 points is ‘many’, 3 points is ‘a little’, and 4 points is ‘almost none’. The stress level then was divided into three categories (a lot of (1-2 points), a little (3 points), and almost no (4 points)). The item values in the questionnaire were applied as they are. Lower scores indicate higher stress perception.
3. Oral examination-related variables
Oral examinations were directly investigated by the dentist. The masticatory level of the participant was surveyed using 5 points Likert scale. The number of residual teeth was used as a variable for determining the tooth condition. The teeth denoted as ‘Decayed missing tooth surface’ marked with ‘4’, ‘Non-decayed missing tooth surface’ marked with ‘5’, ‘un-erupted tooth surface’ marked with ‘8’ were changed to be marked as ‘0’ and were regarded as having no teeth. The other teeth denoted by 1, 2, 3, 6, and 7 were marked as ‘1’ [19]. The number of each tooth was then summed and the total number of teeth was divided into 2 groups (<20, ≥20) [20]. The chewing levels were assessed on a 5 point scale (very uncomfortable, uncomfortable, fair, comfortable, very comfortable) using questionnaires. The chewing levels were divided into two groups: ‘poor’ group of 1-2 points and ‘good’ group of 3-5 points. The item values in the questionnaire were applied as they are.
4. Statistical analysis
Data were analyzed using complex samples. Frequency analysis was conducted to determine the distribution of stress and the general characteristics according to the oral health status. Linear regression analysis was performed to determine the differences between the general characteristics and the oral health condition according to the degree of stress. In addition, logistic regression analysis was conducted to investigate the effectiveness of stress on the residual teeth and chewing level. This study was analyzed using the SPSS (SPSS 23.0 for windows, IBM, USA) program and the statistical significance level was set to 0.05.
Results
1. Characteristics of the participants according to stress
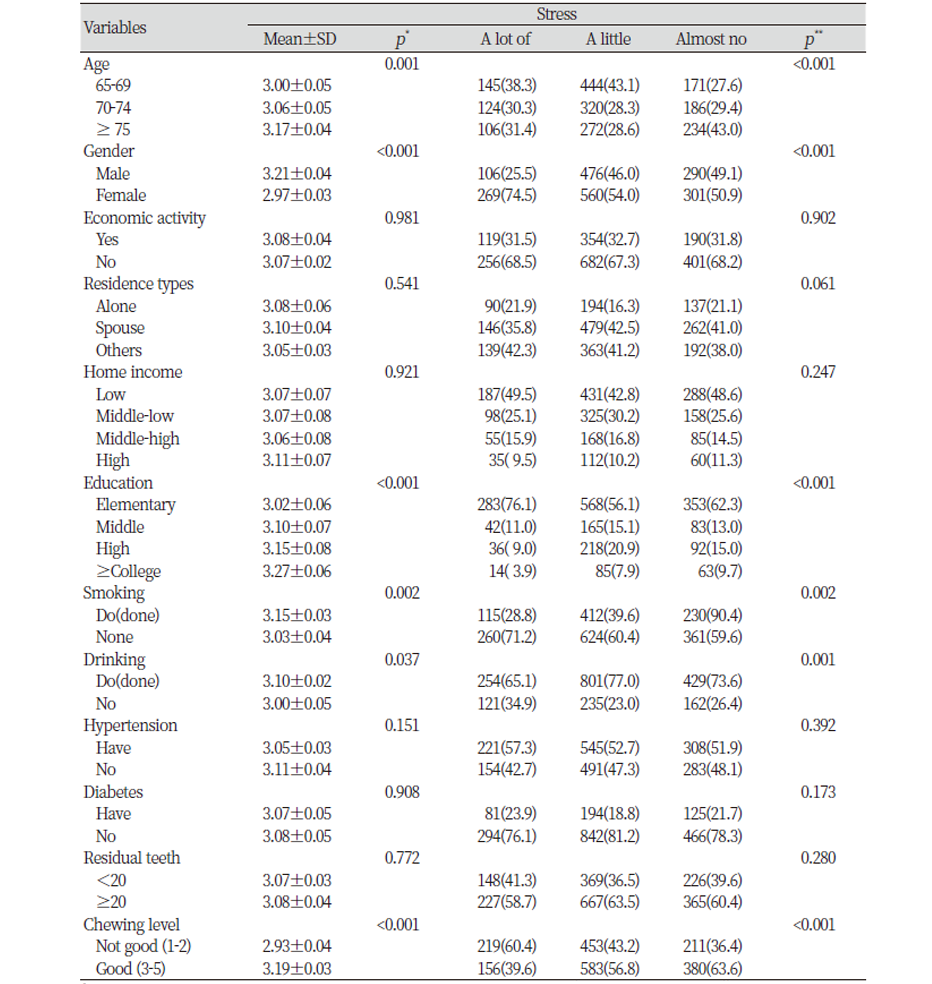
The stress level of the elderly was 3.00 ± 0.05 in the 65-69 years group, 3.06 ± 0.05 in the 70-74 years group, and 3.17 ± 0.04 in the 75 years and older group. The older group (≥75) had lower stress levels. The lower the education level, the higher were the stress levels. The degree of chewing was divided into the ‘not good’ and ‘good’ groups, and the degree of stress was estimated to be higher in the ‘not good’ group than in the ‘good’ group with a statistically significant difference (p<0.05). When the degree of stress was divided into three groups, ‘a lot of’, ‘a little’, and ‘almost no’, there were statistically significant differences in the age, gender, education, smoking, drinking, and chewing (p<0.05) <Table 1>.
2. Characteristics of the participants according to oral health status
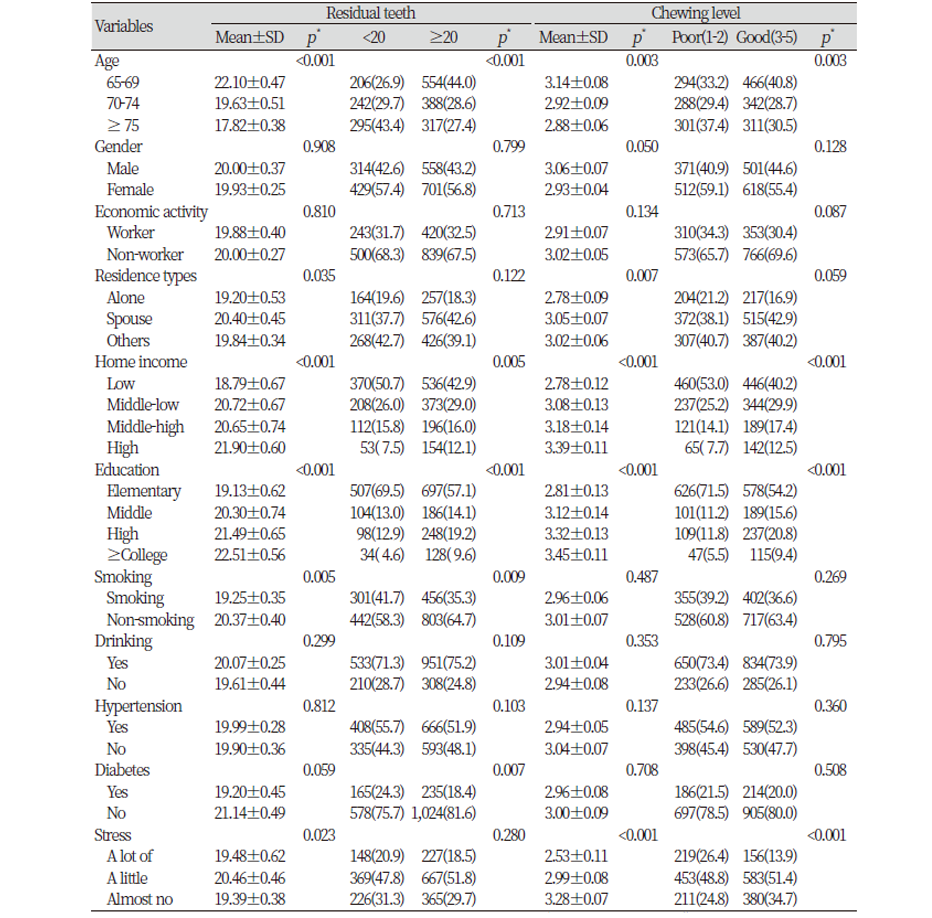
The older the elderly living alone, the lower the household income, the lower the education level, and the fewer teeth remaining in the smoker. There was also a significant difference in the number of residual teeth according to the degree of stress. In addition, the higher the age, the lower the household income, the lower the education level, and the higher the stress, the worse was the degree of mastication. The two groups with <20 or ≥20 residual teeth showed statistically significant differences in the age, home income, education, smoking, and diabetes (p<0.05). The two groups with ‘not good’ or ‘good’ chewing levels showed significant differences in the age, household income, education level, and stress (p<0.05) <Table 2>.
3. Association between stress and oral health status
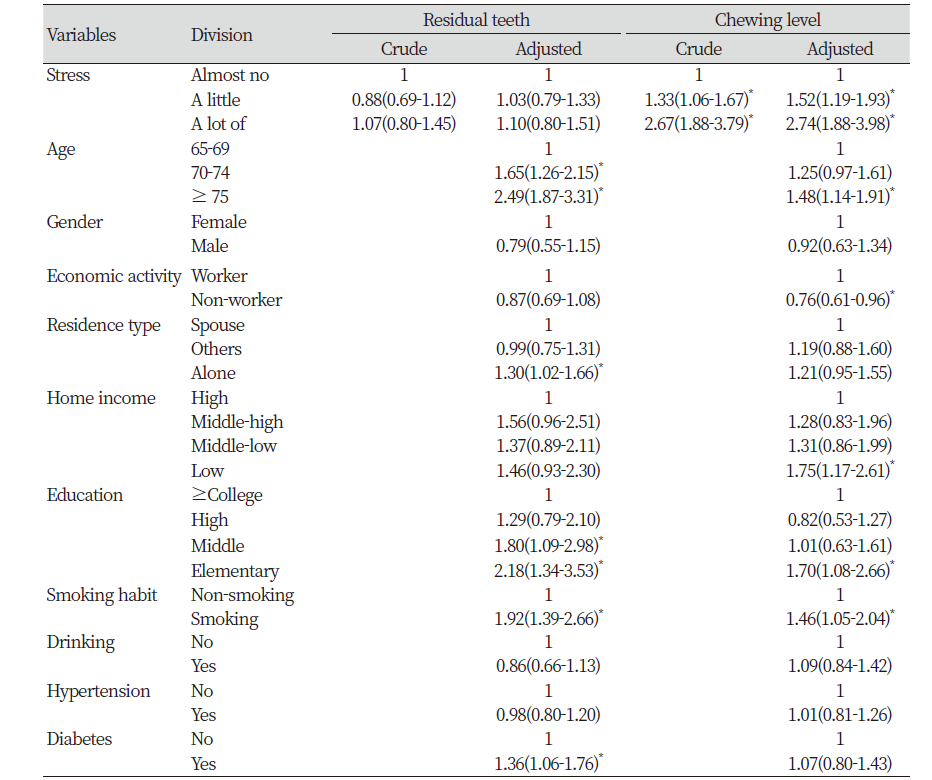
The odds ratio of the poor chewing level was 1.33 times higher in the ‘a little stress’ group than the ‘almost no stress’ group and 2.67 times higher in the ‘a lot of stress’ group than the ‘almost no stress’ group, which was statistically significant (p<0.05). In addition, after adjusting for the age, gender, economic activity, residence type, home income, education, drinking or smoking, hypertension and diabetes. The odds ratio of the poor chewing level was 1.52 times higher in the ‘a little stress’ group than the ‘almost no stress’ group and 2.74 times higher in the ‘a lot of stress’ group than the ‘almost no stress’ group, which was statistically significant (p<0.05) <Table 3>.
Discussions
Lee and Yoon [8] examined the stress level according to various general characteristics and reported that the higher the education level and the higher the household income, the higher was the stress level. However, Cho et al. [21] reported that the lower the educational background and the lower the household income, the more severe was the stress level.
The increased average lifespan has resulted in serious social problems like early retirement of the aging population, which and lead to depression or a sense of alienation due to the increased time spent in isolation physical and mental damage. And the natural death of those around them can be a major stressor for the elderly [22]. Since stress can accumulate negative emotional states such as anxiety and depression, a countermeasure is needed [23]. Although the correlation between stress and various diseases has been previously studied, no clear solution has been found [24]. In order to relieve the stress of the elderly, there are various programs related to the community as well as the individual. In this regard, it is thought that everyone should be interested so that the elderly can share information with each other.
In addition, negligence of oral health due to stress can increase the incidence of oral diseases like dental caries and periodontitis, which can make the chewing and swallowing of food uncomfortable, and also interfere with daily life due to abnormal taste and difficulty in pronunciation [25]. Conditions like excessive mental strain or stress can increase the prevalence of oral conditions, including dry mouth, oral mucosal disease and halitosis [26]. Decreased salivary flow in the elderly causes bad breath, which in turn can cause mental damage in the form of psychological atrophy and anxiety and thus, result in stress and lead to social avoidance and disrupt interpersonal relationships [27]. Cho et al. [19] investigated an association between stress and the number of residual teeth in adults over 40 years old, there was no significant difference between stress and the number of residual teeth, as in this study (p>0.05). Rai et al. [28] reported that salivary stress markers and stress were significantly related with periodontal disease, and ignoring to brush teeth during stress was related with missing teeth.
Roohafza et al. [18] reported that masticatory ability was significantly correlated with depression, anxiety , and stress. Furthermore males reported significantly higher level for masticatory ability than females. And they reported that participants with higher score of anxiety, depression, and stress suffer lower masticatory ability. Petrowski et al. [29] reported that psychosocial stress was related with an rise in chewing frequency measured with sound-based devices.
The discomfort in chewing was found to affect not only the oral health but also the overall quality of life. Poor chewing ability in the elderly can decrease their ability to perform daily activities, thus worsening their quality of life and increasing the occurrence of mental illnesses such as depression [30]. And Miyake et al. [31] reported that chewing attenuates morphologic changes and stress-induced functional in the hippocampus. Therefore, it is necessary to overcome the discomfort in chewing function.
This study was based on the National Health and Nutrition Survey to represent the elderly in Korea. However, because this study is a cross-sectional study, it can’t explain the causal relationship whether the chewing level is uncomfortable due to high stress, or whether it is more stressed due to the uncomfortable chewing level. And even after adjusting covariates the value was increased seems that there was a difference in the number of subjects. In addition, there were limitations because it was investigated using subjective measuring tools for stress and chewing level.
Therefore, more objective measurement tools need to be utilized and more in-depth follow-up studies are needed.
Conclusions
This study was examined their stress level and chewing ability from elderly people over 65 years old using the 2nd and 3rd year (2014-2015) of the 6th Korea National Health and Nutrition Examination Survey data. The results are below.
1. The degree of stress according to the general characteristics was significantly different in age, gender, education, smoking, drinking, and chewing level (p<0.05).
2. The chewing level according to general characteristics was significantly different in age, income(home), education, and stress (p<0.05).
3. The stress in the elderly is related to the chewing level. When there was a lot of stress, The odds ratio of poor chewing level was 2.67 times, and the risk ratio was 2.74 times after adjusting age, sex, residence types, economic activity, home income, education, smoking, drinking, hypertension, diabetes.
We hope to improve the overall quality of life of older adults by exploring various methods to reduce the stress of the elderly and also focusing on oral health as well as general health. This study is expected to be a useful resource for improving mental health and oral health in the elderly.

