Introduction
Early childhood caries (ECC), which is the most representative oral disease occurring in childhood, are infectious and occur simultaneously, leading to a sudden increase of dental caries in children [1]. According to the results of the 2018 Child Oral Health Survey, 68.5% of old children aged 5 experienced primary caries on an increasing trend, and 32.3% of children who had not been treated with more than two primary teeth were shown to require treatment [2]. As the importance of oral health management is being emphasized [3], more attention needs to be paid to oral health management, and in particular, parents should pay attention to the oral health management of their children [4]. Most studies have reported that the knowledge, attitude, and oral care behaviors of the parents affect the oral health status and behavior of the children [5-8]. In addition, oral health education experience [9] and parents’ understanding of oral health information [10,11] affected the oral health status and behavior of children. Most previous studies have focused on the static correlation between parents and children through surveys, and evaluation of oral care programs in which both the parents and children participate together is lacking [5-9]. In Ahn et al.'s study [12], a questionnaire survey, oral health education, and dental plaque test were performed for three weeks on 130 children aged 3-5 and their parents, and it was observed that the oral health management behavior and dental plaque tests results of the children were positively improved. As such, previous studies evaluated programs to prevent dental caries; however, the same program was applied to the subjects, and individual differences were not compared. In 2002, Caries Management by Risk Assessment (CAMBRA), which is a method to systematically manage caries in accordance with appropriate guidelines after assessing the risk of caries in individual patient, was first introduced by Dr. Featherstone [13,14]. CAMBRA evaluates the risk of caries based on risk factors, protective factors, and disease indicators for each patient into extreme high, high, moderate, and low risk [15]. In Korea, Lee [16] and Cho [17] introduced a program using CAMBRA; however, it was not widely used in clinical practice despite being a clinically excellent and suitable tool to effectively prevent ECC. CAMBRA-kids was recently developed by modifying CAMBRA, which is an individual patient-centered and evidence-based caries management program. CAMBRA-kids enables systematical management of dental caries in children under the age of 5 who have a high risk of caries [18]. The application automatically determines the risk level when the parents and clinicians enter the required items. This tool provides appropriate management methods for the risk groups of the children to the parents, and it can also increase the interest of parents in the oral care of their children. Various applications using wearable and smart devices have recently been developed and have led to increased interest and use of mobile healthcare [19]. In Lee’s study [20], a program that monitored tooth brushing education for children at home through a smart device (Mom brush) was used, and positive effects were observed compared to the conventional, simple, and repetitive oral health education conducted at educational institutions. As smart devices are being used more actively in oral health care, applications related to oral care such as Panda Toothbrushing, My brush, Brush DJ, Brush Monster, and Brushing Hero can be downloaded from Google Play and App Store. However, the majority of these applications are games using characters and offer simple brushing methods, oral management information, and timer functions.
There was a lack of studies that applied oral health education and management programs through a communication method between experts and the general public using an application, and most previous studies mainly provided knowledge and information on oral care.
Therefore, the CAMBRA-kids application was used in children under the age of 5 and their parents to evaluate oral health knowledge, oral care self-efficacy, oral care performance rate, and parents’ satisfaction with the program to provide basic data for increased oral health.
Methods
1. Subjects and data collection
This study was conducted from September 2018 to October 2019. The purpose and contents of the study were explained to the head of the institution, and two institutions that agreed were selected based on the convenience of access. The study subjects were children under the age of 5 who were enrolled at the relevant institution and their parents. After explaining the purpose and the progress of the study, those parents and children who agreed to participate were included. G*power 3.1.9.2 program was used to calculate the sample size with an effect size of 0.25, significance level of 0.05, and a power of 0.80. As a result, a total of 101 subjects were required. Considering the dropout rate, a total of 166 were selected. A total of 47 subjects were withdrawn from the study (27.7% dropout rate), and 119 subjects were included in data analysis. This study was conducted after approval of the Institutional Review Board of 00 university (IRB, NSU-1041479-007).
2. Research tools
1) CAMBRA-kids application
Kang and Lee [18] developed the CAMBRA-kids application in 2019 for systematic management of dental caries in infants, and the waterfall model of system development life cycle was used to develop the software, which consisted steps of analysis, design, execution, evaluation, and maintenance. Content validity and understandings of the Korean version of dental caries evaluation tool were assessed and revised. Satisfactory results were observed, confirming that the tool could be used to measure the risk of caries.
2) Oral health knowledge
Items of oral health knowledge for parents of preschool children, which was developed in 2013 by the Oral Health Team of the Korea Health Promotion Foundation, was used as a reference, and the tool, which was reconstructed by Lee [21], was revised and supplemented for the current study. “Correct answers” and “incorrect answers” were scored 1 and 0, respectively, and a higher score indicated a high level of oral health knowledge of the parent. In a previous study, Cronbach's alpha was 0.753, and in the current study, it was 0.689.
3) Oral health self-efficacy
Oral health self-efficacy refers to behavioral techniques that enable effective behavior changes by acquiring information and motivation, and this study used the Self-Efficacy Scale for Self-care (SESS) tool, which was originally developed by Kakudate [22] and modified by Kim [23]. The tool consisted of 15 items, which were evaluated on a 5-point Likert scale with “not confident at all”, “not confident”, “neutral”, “confident”, and “very confident”, and a higher score indicated higher self-efficacy. In the study by Kim [23], Cronbach's alpha was 0.841, and in the current study, it was 0.914.
4) Satisfaction with the program
The response evaluation and measurement tool among Kirkpatrick’s four-level evaluation model [24], which was modified by Shin et al. [25] through validation with experts and used by Lee [26], were modified and supplemented. The tool, which was modified to eight items, was evaluated on a 5-point Likert scale with “strongly disagree”, “disagree”, “neutral”, “agree”, and “strongly agree”. A higher score indicated a higher level of satisfaction. Cronbach's alpha was 0.912 and 0.911 in the previous study [25] and in the current study, respectively.
3. Research procedures
The research contents were explained to the heads of the two institutions who agreed on the purpose of the research and to the children and their parents. Informed consents were obtained from every subject, and a written explanation of how to use the application was provided. Additionally, a questionnaire was distributed to the parents to assess their general characteristics, oral health knowledge, and oral care self-efficacy.
The parents were asked to download the CAMBRA-kids application, sign-up, and log-in. On the first main screen, CAMBRA-kids was introduced with a phrase “A Caries Risk Management Program for Infants”. The parents were asked to enter the risk factors and protective factors of their children, and the clinician entered the disease index after conducting a clinical examination on the children. “Risk factors” included caries that occurred within the last 12 months, three or more snacks a day, factors that reduce saliva, developmental disorders or other diseases related to growth, need for special health care, and types of health insurance. “Protective factors” included fluoride compounds or fluoride supplements, use of fluoride-containing toothpaste, use of fluoride varnish within the last six months, regular oral examination, and xylitol intake. “Disease indicators”, which was evaluated by the clinician, included white spots in the oral cavity, clear caries, past experience of caries, dental plaque attachments, and remarkable saliva secretion. Once every item was entered on the application, the risk level of caries was automatically determined by an algorithm based on risk factors, protective factors, disease index, and special relevant data [18]. The children’s caries risk group were provided to the parents, and appropriate management methods for each risk group through the application, and images of the oral cavity, results of caries causative bacteria, dental plaque, mineral nitrogen loss, and saliva secretion, and comments by the clinician were available on the mobile application.
After 12 months, the same questionnaire, which was provided during the preliminary survey, was sent to the parents to assess their oral health knowledge and oral health self-efficacy for the children, and an additional questionnaire was provided to assess parents’ satisfaction level with the program.
4. Data analysis
The collected data were analyzed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA) statistics program at a significance level of 0.05.
Descriptive statistics, paired t-test, and one-way analysis of variance (ANOVA) were performed to evaluate the general characteristics of the subjects, changes in oral health knowledge and oral care self-efficacy of the parents after the program, and the level of satisfaction with the program. Additionally, the Scheffe test was performed for post-hoc analysis.
Results
1. General characteristics of subjects
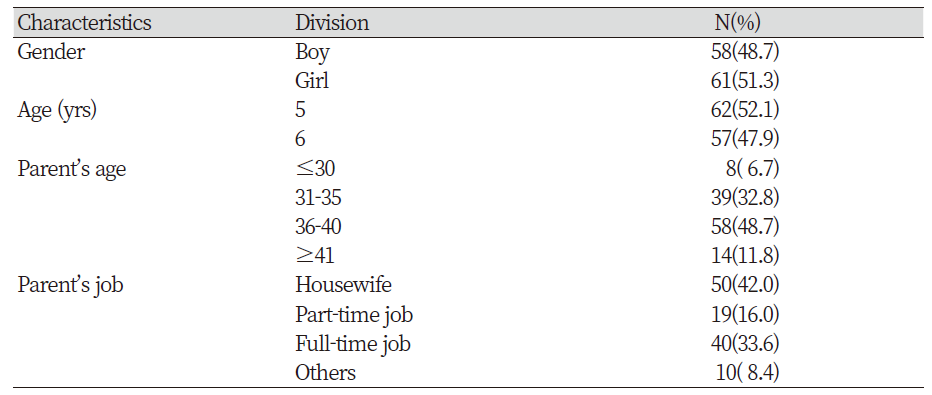
A total of 119 subjects were included in the study; 51.3% were girls and 48.7% were boys. A total of 52.1% were 5 years old and 47.9% were 6 years of age. For the parents, 48.7% were between the ages of 36 and 40, and the mean age was 39.3 years. For occupation, the greatest number of parents were housewives at 42.0% <Table 1>.
2. Changes in the risk level of caries of children
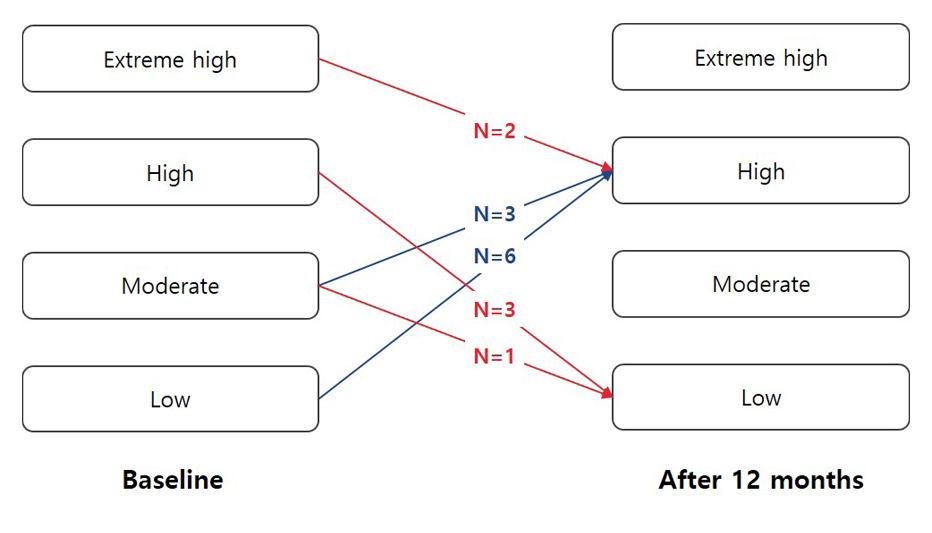
After the 12-month long caries management program, the risk of caries in children decreased by 22.2%, 57.1%, and 9.5% in the extreme high- risk, moderate- risk, and low -risk groups, respectively. In contrast, the risk of caries increased by 9.8% in the high- risk group. For detailed changes in caries risk groups, six children from the low risk group at the beginning of the study moved into the high -risk group after 12 months while three children from moderate- risk group were moved to the high- risk group. On the other hand, two children moved from the extreme high- risk group to high risk group, three from the high- risk group to low- risk group, and one from the moderate- risk to low risk group <Fig. 1>.
3. Changes in self-efficacy of parents for oral care of children
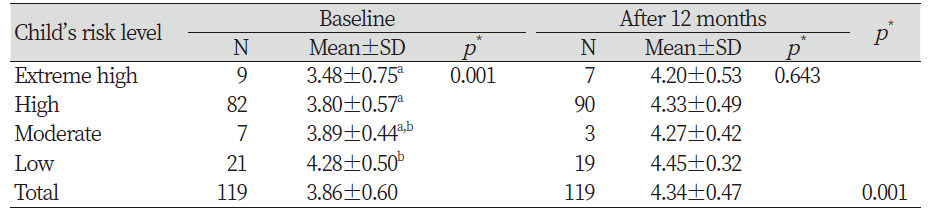
Self-efficacy of parents for oral management of children increased significantly from 3.86 at the beginning of the study to 4.34 after 12 months (p<0.001). Additionally, there was a statistically significant difference in the self-efficacy of parents according to the risk of caries in the children (p<0.05), and post-hoc analysis revealed that those parents whose children were in the low-risk group had a higher self-efficacy than those whose children were in the high and extreme high-risk groups. After 12 months of the program, self-efficacy had increased in all risk groups, and there were no statistically significant differences between each risk group <Table 2>.
4. Changes in oral health knowledge of parents
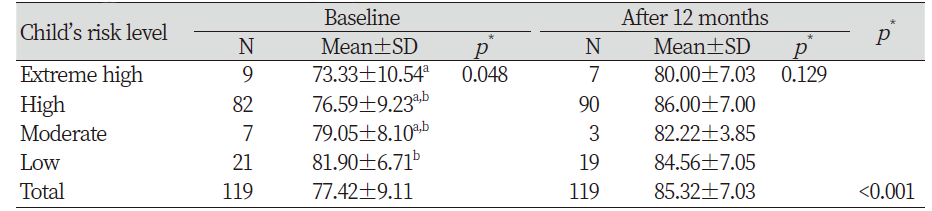
Oral health knowledge of all subjects increased significantly from 77.42 at the start of the study to 85.32 after 12 months (p<0.05). There was a significant difference in parents’ oral health knowledge depending on the caries risk group of the children (p<0.05), and post-hoc analysis revealed that the parents whose children were in the low-risk group had higher oral health knowledge than those whose children were in the extreme-risk group. However, there was no significant difference in the oral health knowledge of parents according to the caries risk group of children after 12 months <Table 3>.
5. Level of parental oral care performance according to caries risk
During the program, oral care management strategies for each risk group were provided to the parents via the mobile application, and the level of oral care performance by the parents was indicated from 1 to 5 points. Those parents whose children were in the extreme high-, high-, and moderate-risk groups had a score of 2.60, 3.34, and 2.93, respectively, and parents whose children were in the low-risk group had the highest score at 4.12 <Table 4>.

6. Parents’ satisfaction with the program
After the end of the program, parents whose children were in the low risk group had the highest satisfaction score at 4.03, and those whose children were in the extreme high, high, and moderate risk groups showed a satisfaction score of 3.94, 3.80, and 3.67, respectively <Table 5>.

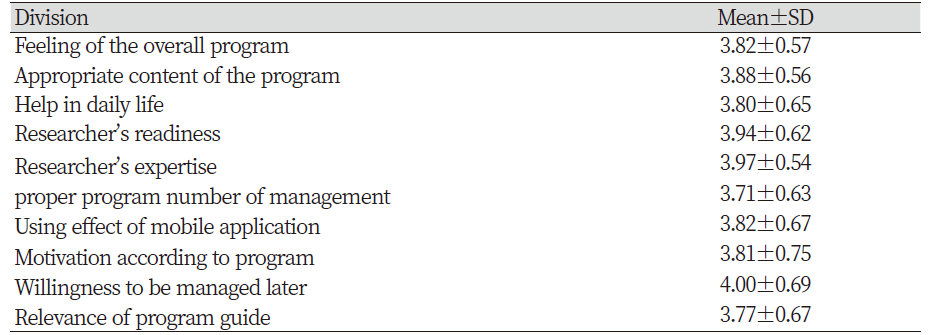
The item “Do you intend to use the program if a similar caries management program like CAMBRA-kids is available next time?” had the highest satisfaction score, followed by “Did the researcher of the caries management program have sufficient expertise and qualities?” In contrast, the item on the appropriate number of caries management program showed the lowest satisfaction score <Table 6>.
Discussion
In this study, a mobile application program was used for a 12-month systematic management of dental caries. and changes in the caries risk level in children and self-efficacy for oral care, oral health knowledge, oral management performance, and program satisfaction of the parents were assessed.
At the beginning of the study, caries risk group was assessed for each participant, and after 12 months of the program, changes in the caries risk group were evaluated. In a previous study [27], only 2% of children were assigned to the extreme high-risk group and thus, those children were included in the same group as those in the high- risk group. In the current study, one of the institutions was a public kindergarten that conducted special classes, and children in the extreme high- risk group were available. Therefore, these children were evaluated separately from the high- risk group in our study. The number of children in the extreme high -risk group decreased from nine at the beginning of the study to seven after 12 months. The mothers of two children whose caries risk level changed from extreme answered yes to the item on factors of reduced saliva among disease indicators in the preliminary questionnaire. At the end of 12 months, these mothers did not answer to this item, which seemed to have led to such result where the number of children in the extreme high- risk group decreased from nine to seven. However, the reason for this answer was personal information, and therefore, further investigations could not be pursued. A total of three children were moved from the high- risk group to the low risk group after 12 months. For these children, the item “mother or main caregiver had caries that had progressed in the last 12 months”, which is one of the risk factors, was answered yes at the beginning of the study. After 12 months, the item was not answered as yes, and other items of risk factors excluding dental plaque were also not answered as yes, which caused their risk levels to decrease. In addition, progressed caries were observed at the beginning of the study in the three children. During the 12 months of the program, those caries were treated, which seemed to have changed their risk group to the low risk group.
In contrast, six and three children in the low-risk group and moderate-risk group, respectively, were re-assigned to the high-risk group after 12 months of the program. Among these children, four were moved to the high-risk group as it was indicated that “parents had caries that have progressed in the last 12 months”, and the other five children “currently have restored teeth” or “clear caries are observed in the oral cavity”, which increased their risk level. Moreover, there was a slight increase in the number of newly developed caries in the low- and moderate-risk groups compared to the extreme high -and high-risk groups. Featherstone et al. [27] observed that the number of new caries increased in all caries risk groups after two weeks, which was significantly higher in the high-risk group. In childhood, the incidence of dental caries is high, and permanent teeth begin to erupt in the mixed dentition stage, requiring more attention to oral care [28]. Therefore, there was a limitation to evaluating the effects of the program due to changes before and after the program in the risk groups.
Self-efficacy of parents for oral management of children was increased significantly from 3.86 at the beginning of the study to 4.34 after 12 months. At the beginning of the study, parents whose children were in the low-risk group showed a significantly higher level of self-efficacy than those whose children were in the high- and extreme-risk groups. However, self-efficacy of parents was increased in all risk groups after 12 months of the program. Choi [29] observed that parents’ self-efficacy for oral health management of children was increased after four weeks of an oral health program. Although an oral health education program was not provided in the current study, it seems that similar effects were observed as knowledge was provided through the mobile application, which changed perception of oral health and motivated the parents to further care for the oral health of their children.
Lee [30] reported that the oral health behavior of children was positively correlated with the oral health knowledge of the parents, affecting prevention of dental caries in the children. In the current study, oral health knowledge of parents increased from 77.42 at the beginning of the study to 85.32 points after 12 months. At the start of the study, parents whose children were in the low-risk group had higher oral health knowledge than those whose children were in the extreme-risk group. However, oral health knowledge of parents of children in all risk groups was increased after 12 months of the program, and there was no difference between the risk groups. In particular, those parents whose children were in the high-risk group had the highest oral health knowledge after 12 months. During the program, the results of clinical examinations were provided to parents whose children were in the high-risk group every three months, which seemed to have helped the parents to gain knowledge on oral health information. In the moderate- and low-risk groups, clinical examinations were performed every 6 and 12 months, respectively, and feedback was provided through the mobile application. After 12 months, the parents’ oral health knowledge had increased; however, there was no significant difference between parents of different risk groups. In Choi's study [27], only fragmentary knowledge of oral health was provided via text messages or booklets to promote oral health knowledge and behavior in mothers, and thus, Choi suggested development of a web-based program using a smart phone and evaluation of the effects of the program.
After completing the 12-month long dental caries management program, parents’ satisfaction with the program was evaluated. The average satisfaction score for the subjects was 3.84 points, and satisfaction was high in the order of low-, extreme high-, high-, and moderate-risk group; however, there was no significant difference. The parents whose children were in the low-risk group showed the highest level of satisfaction as well as self-efficacy and oral health knowledge at the beginning of the study and the highest oral care performance level after 12 months of the program. It is thought that those parents were already interested in oral care, thereby having greater knowledge and self-efficacy and showing a high level of satisfaction with the program. When individual items on satisfaction were assessed, the item “Do you intend to use the program if a similar caries management program like CAMBRA-kids is available next time?” had the highest satisfaction score. Through the course of this study, children were given an opportunity for systematic management of dental caries. Children underwent dental plaque test, caries activity test, and fluoride varnish treatment by experts and received 1:1 training on brushing techniques according to the guidelines for each risk group. The current study showed satisfactory accessibility as it was conducted in a kindergarten or daycare center, and information on tests results, pictures, and comments by the clinician were easily accessible by parents on the mobile application, which seemed to have contributed to the high level of satisfaction with the current study.
This study evaluated children’s caries risk group, and a systematic management of dental caries was performed for each group using a mobile application. The overall caries risk level was decreased, and positive changes in oral health knowledge of parents and self-efficacy of parents for oral management of their children were observed. However, this study was conducted on 119 subjects, and thus, the results cannot be generalized. Moreover, this study was conducted with a single group with a pre- and post-test design. Therefore, it would be necessary to inlude a control group in subsequent studies to control factors that can affect internal validity.
Conclusions
In this study, dental caries in children under the age of 5 were managed using a mobile application for their parents for 12 months. Oral health knowledge, oral health self-efficacy, oral care performance, and satisfaction of the parents were assessed, and the following conclusions were drawn:
1. The caries risk level in children of the extreme high-, high-, moderate-, and low-risk group decreased by 22.2%, 9.8%, 57.1%, and 9.5%, respectively.
2. Self-efficacy of parents for oral management of their children was higher in those parents whose children were in the low-risk group than in those whose children were in the extreme high- and high-risk groups. After 12 months of the program, self-efficacy for oral management was increased in all risk groups, and there were no statistically significant differences between the groups.
3. Oral health knowledge was higher in parents whose children were in the low-risk group than in those whose children were in the extreme-risk group. However, oral health knowledge of parents was increased in all groups, and therefore, there were no significant differences in oral health knowledge between the risk groups.
4. The level of satisfaction with the program was the highest in the parents whose children were in the low-risk group at 4.04 points, followed by parents whose children were in the extreme high-, high-, and moderate-risk groups.
This study demonstrated that dental caries management in children using a mobile application has positive effects on oral health knowledge, self-efficacy of oral care, oral care performance, and satisfaction in the parents in addition to changes in the caries risk group of the children. Based on these findings, a measure that can be linked with community care for caries management in children would be necessary in the future.

