Introduction
Most dental supplies used during treatment are contaminated with patient blood, saliva, or bodily fluids. Re-using contaminated tools in dental clinics may cause cross-contamination, thereby increasing the risk of viral spread (e.g., hepatitis B virus and human immunodeficiency virus)[1]. Dental supplies must be strictly monitored and used after sterilization, and the use of disposable dental supplies (DDS) is recommended for certain types of equipment and disposables used in the clinic[1].
A few countries (e.g., the United States, Germany, and Australia) have regulations regarding the re-use of DDS; certain DDS can be re-used after appropriate treatment performed by authorized companies[2]. However, a few other countries, including Korea, have partial regulations for specific types of DDS (e.g., prohibiting the re-use of disposable needles/syringes).
The use of DDS in dental clinics, when necessary, is an appropriate infection control protocol for the prevention of cross-contamination. Previous studies investigated the real-world re-use of DDS in a few dental clinics[3-5]. DDS are often designed for one-time usage in equipment that is difficult to sterilize; re-use of these DDS without appropriate sterilization processes can result in dangerous outcomes. Therefore, imprudent re-use of DDS in dental clinics—where invasive interventions often are performed—is inconsistent with the infection control protocol, and may threaten the health and safety of both dentists and patients.
Previous studies that have assessed the re-use of DDS did not actively investigate the real-world re-use of DDS, primarily focusing on retrospective analysis of DDS re-use in a few dental care institutions, as well as the re-use of personal protective equipment (PPE) as an indicator for dental infection control activit.[3-5]. This study aimed to investigate the real-world re-use of DDS in dental clinics, based on the risk levels of each DDS, and to identify the underlying causes of DDS re-use.
Methods
1. Subjects
Dental hygienists working at dental clinics or dental hospitals in Seoul, Incheon, or Gyeonggi province in Korea were selected by using simple convenience sampling, between July 5, 2017 and September 10, 2017. The number of subjects was calculated using the G*power 3.1 program. The total sample size was 210 when the effect size was 0.5, the Aipha-error was 0.05, and the power was 0.95. The minimum sample size was 233 considering the dropout rate of 10%. The total number of subjects was 277, which satisfied the minimum sample size. This study was performed after obtaining approval from the Institutional Review Board (IRB) of Y University in Korea (CR317047). The subjects provided signed informed consent to participate in the study after receiving an explanation of the study purpose.
2. Measures
A structured questionnaire survey was used in this study, assessing the subjects’ general characteristics, awareness of infection control, awareness of DDS management, and re-use of DDS.
1) General characteristics
The subjects’ work experience in clinical settings ranged from 4 months to 32 years and 8 months. For this analysis, subjects were categorized into 3 groups: <2 years, 2–4 years, or ≥5 years of experience. These groupings were based on the results of a previous study, which reported that dental hygienists with 2–4 years of work experience primarily perform infection control-related work[7]. For the type of dental clinic, the centers were categorized as either dental clinics or dental hospitals, based on their size. The average number of daily patients treated by a dental hygienist was dichotomized as ≤8 patients per day or ≥9 patients per day[8].
2) Infection control characteristics
Possession of the dental infection control guidelines was assessed using response options of “Yes,” “No,” or “I do not know”[9]. The awareness of infection control was assessed using a modified version of the infection control awareness assessment tool developed by Lim et al[10], which included 35 questions. The awareness of DDS was assessed with 2 questions; “Manufacturer’s instructions regarding the re-use of DDS should be checked” and “DDS used in a patient should be discarded.” Each question was assessed on a 4-point scale; responses measuring awareness of both infection control and DDS were dichotomized into “not important (1–2 points)” and “important (3–4 points)” for the analysis.
3) Definition and categorization of DDS
According to the infection control guidelines of the Centers for Disease Control and Prevention[1]. DDS are defined as tools that cannot be properly sterilized due to lack of heat resistance, are unable to be properly washed due to physical shape, or can easily undergo change, abrasion, or damage during the treatment process required for re-use. This study included assessments of 9 different types of DDS that are commonly used in dental clinics. Based on their purposes, these DDS were categorized into the following groups: Critical, Semicritical, Noncritical, or PPE[1]. DDS in the Critical group included anesthetic needles, which penetrate through soft or hard tissue during treatment. DDS in the Semicritical group included 5 types of products that do not penetrate through tissue; however, they may come in contact with mucous membranes or damaged skin. These included prophylaxis cups, plastic saliva ejectors, irrigating syringes, plastic orthodontic brackets, and fluoride trays. DDS in the Noncritical group included the products that come in contact with healthy skin; surface barrier film was the only product in the Noncritical group. Lastly, PPE comprised tools to protect both dentists and patients from blood and pathogenic/infectious material; these included masks and gloves.
4) The real-world re-use of DDS
Response options regarding the re-use of these 9 different types of DDS included “No re-use,” “Re-use,” or “No use at all.” The proportion of subjects who responded “Re-use” was calculated.
3. Statistical analysis
The general characteristics of the subjects and the real-world re-use of DDS were analyzed using frequency analysis and the chi-squared test. All statistical tests were performed with SPSS Statistics 18.0 (IBM Co., Armonk, NY, USA); the significance level was set at 0.05.
Results
Assessment of the real-world re-use of DDS, with respect to the subjects’ general characteristics, showed that, overall, 89.5% of the subjects were re-using DDS; subgroup analysis showed the following proportions of specific DDS re-use: 63.9% were re-using DDS in the Semicritical group, 66.4% were re-using PPE, 19.5% were re-using DDS in the Noncritical group, and 1.8% were re-using DDS in the Critical group. Based on the type of clinic, the rate of re-use of Semicritical group was higher in dental clinics, compared with dental hospitals (0.001) <Table 1>. In addition, the frequencies of the re-use of DDS in the Semicritical group and the re-use of PPE were relatively higher in the dental hygienist group with an average number of daily patients of ≤8 <Table 1>.
Subjects who had infection control education (training) in the previous 2 years exhibited higher frequency of DDS re-use in the Semicritical (97.1%) and Noncritical groups (25.7%), compared with subjects who did not have infection control education. Subjects working at clinics without infection control guidelines exhibited a relatively higher frequency of the re-use of DDS in the Semicritical group (90.6%) and the re-use of PPE (83.0%) (0.001)<Table 2> .
Associations between the re-use of DDS and the clinical work experience, awareness of infection control, or awareness of DDS management were not investigated.
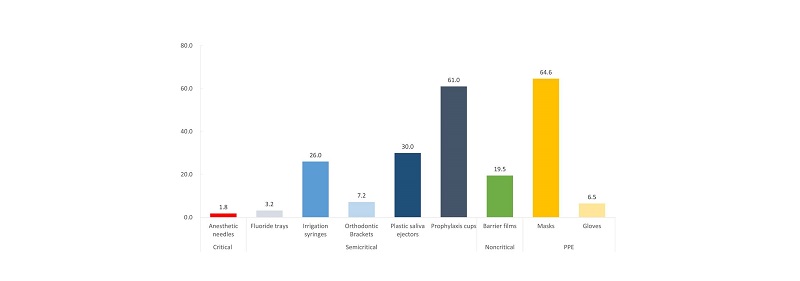
The most frequently re-used type of DDS, among the 9 types assessed, was masks (64.6%), followed by prophylaxis cups (61.0%) and plastic saliva ejectors (30.0%) <Fig. 1>.
Discussion
DDS should be appropriately discarded after being used in a single patient[1]. However, all 9 types of DDS assessed in this study were re-used to different extents <Fig. 1>. The rate of re-use for anesthetic needles, which are in the Critical group, was 1.8% <Fig. 1>; this exceeded the percentage of dentists’ re-using the needles (1.5%) in a previous study by Oosthuysen et al[11]. The re-use of needles must be avoided in all circumstances, because multiple viruses (hepatitis B and C, and HIV) can be transferred via such re-use[1,12]. However, World Health Organization has estimated that approximately 40% of the needles and syringes worldwide are re-used without sterilization[12]. The regions most affected by needle reuse are Africa, Eastern Mediterranean Europe and Southeast Asia[13]. Despite clear statements prohibiting the re-use of disposable needles (including disposable anesthetic needles) in the infection control guidelines of a variety of countries worldwide[1,14,15], a subset of dental practitioners continue to disregard this regulation; this is an important issue that requires serious attention and consideration.
Among DDS in the Semicritical group that were assessed in this study, the proportions of hygienists who reported re-use were highest for prophylaxis cups (61.0%) and plastic saliva ejectors (30.0%) <Fig. 1>. In most cases, prophylaxis cups and plastic saliva ejectors are packaged in bundles. In Korea, DDS packaging is legally required to state “disposables” or “do not re-use”[16]; however, when the individual items are removed from packaging, they may not have such labels, resulting in confusion. Furthermore, prophylaxis cups and plastic saliva ejectors, depending on the treatment and their specific use during treatment, can appear to be exceptionally clean after washing and undergoing an appropriate sterilization process, without significant functional issues; therefore, there is an increased chance that these products might be re-used. The recommended sterilization protocol commonly used in dental care institutions worldwide is autoclave sterilization[3,17] ; therefore, products made with plastic or rubber may exhibit an altered shape after sterilization. The requirement for safe re-use of DDS is the absence of functional and physical damages after sterilization[18]. For example, in a previous study that assessed the contamination of dental burs sterilized after patient treatment, contaminants were found in the cracks of the burs. Therefore, dental burs were categorized as a tool that could not be completely washed and sterilized; moreover, dental burs were recommended for disposal after the initial use, although the tool could be sterilized[19]. Long and narrow tubes in the disposable plastic saliva ejectors and fine cracks inside the prophylaxis cups are difficult to completely wash and sterilize. Furthermore, other DDS products, including irrigating syringes, plastic orthodontic brackets, and fluoride trays, cannot be appropriately processed for re-use due to their physical shape and the characteristics of their raw materials.
Barrier film is recommended for the surface areas of equipment that is difficult to clean, as well as light handles and switches, stool controller, and buttons with radiation exposure. A new film should be used for each patient[1]. Reynolds et al[20] reported that 80% of cross-contamination occurs via hand contact. The barrier film had a re-use rate (no exchange after one-time use) of 19.5% <Fig. 1>; the rate of re-use was higher in dental hospitals (25.7%) than in dental clinics (6.4%) <Table 1>. The proportions of clinics that did not utilize barrier films were 12.0% and 27.7% for dental hospitals and dental clinics, respectively. The rate of re-use for barrier film was higher in the clinics that possessed an infection control guideline (25.9%) and had an average number of daily patients of ≥9 (39.1%). Medical costs related to the use of barrier film are affected by the number of patients, as well as the number and size of covered surfaces[21]. Previous studies suggest that time and medical cost are barriers to compliance with infection control, which could partially explain this phenomenon[22,23].
The rate of mask re-use was the highest at 64.6% <Fig. 1>. In general, wet masks exhibit reduced protection against blood-mediated pathogens and other infectious bacteria. Therefore, even during treatment, wet masks should be immediately replaced[1]. However, in patients with lower risk of mask contamination (e.g., dental examinations) or no wetting of masks, replacing the mask for each patient may not be necessary. Because “re-use” in this study was defined as re-using DDS after their initial use, the findings of this study are limited in their ability to explain the appropriateness of mask exchange for every patient.
The infection control guideline can serve as a standard for systematic infection control activity[1]. Compliance with the infection control protocol was greater among dental hygienists with knowledge of infection control, as well as those working at clinics with dental infection control guidelines[22,24]. Previous studies have reported widely differing values (27.6–82.6%) regarding the percentage of dental care institutions with infection control guidelines[11,24,25]. In this study, the percentage of dental clinics or hospitals with infection control guidelines was 61.4%; however, 84.7% of these clinics were re-using 1 or more DDS <Table 2>. The dental infection control guidelines used in dental clinics worldwide suggest that most DDS should not be re-used[1,14,15]. However, specific standards or criteria for DDS and the risks from the re-use of DDS are not fully described; thus, these should be supplemented with additional information[1,14,15].
|
Table 1. Real-world re-use of disposable dental supplies, according to the subjects’ general characteristics 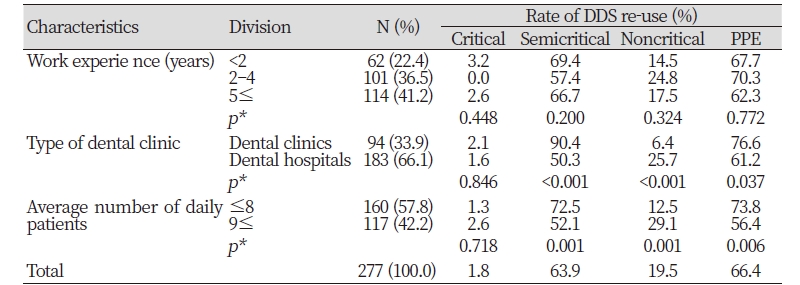
|
|
|
*by chi-squared test or Fisher’s exact test |
|
|
Table 2. Real-world re-use of disposable dental supplies, according to infection control characteristics 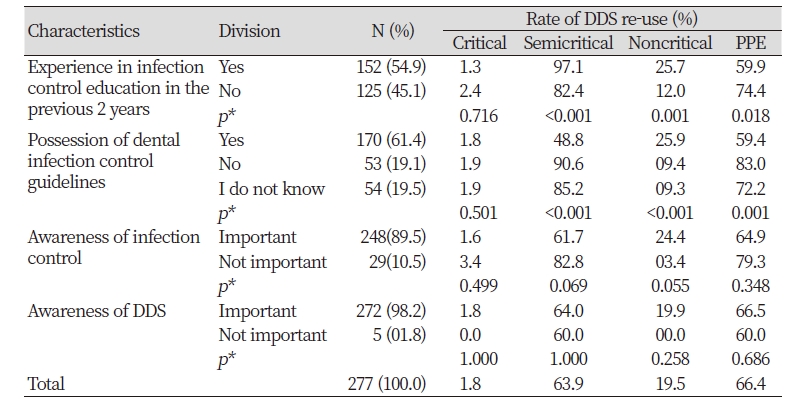
|
|
|
*by chi-squared test or Fisher’s exact test |
|
In this study, the rate of re-use of Critical group, Semicritical group and PPE was higher in dental clinics, compared with dental hospitals <Table 1>. Compared with dental hospitals, dental clinics often do not have infection control guidelines and exhibit low compliance with infection control protocols[25] ; this observation was confirmed in our study, with 76.0% of dental hospitals and 33.0% of dental clinics possessing infection control guidelines. Kim et al[3] and Choi and Kim[26] reported that larger hospitals have dedicated personnel for infection control and receive economic support for infection control.
Abreu et al[27] reported that the awareness of infection control has an impact on compliance with infection control activity. However, the outcomes of this study showed no significant association between the rate of re-use of DDS and the awareness of either infection control or DDS management.
Regarding awareness of infection control and DDS management, 89.5% and 98.2% of the subjects responded that infection control and DDS management are important <Table 2>. Thus, the re-use of DDS may be caused by inappropriate or nonexistent guidelines, or by habitual practice, rather than as a result of the awareness or attitude of dental hygienists.
This study has limitations that should be acknowledged. First, we only assessed a few types of DDS used in dental offices and surveyed dental hygienists in some areas. Therefore, it is difficult to generalize the finding of this study to the overall Korean dental offices. Second, the study findings are limited in their ability to explain the appropriateness of mask exchange for every patient. However, this study assessed the characteristics of dental clinics and dental hygienists with respect to the real-world re-use of DDS, in order to more clearly determine the need for attention and development of guidelines for this issue.
Conclusions
This study aimed to investigate the real-world re-use of DDS in dental clinics, based on the risk levels of each DDS, and to identify the underlying causes of DDS re-use. A total of 277 dental hygienists were respond questionnaire survey and this study conclusions were as follows.
1. 89.5% of the subjects were re-using DDS; subgroup analysis showed the following proportions of specific DDS re-use: 63.9% were re-using DDS in the Semicritical group, 66.4% were re-using PPE, 19.5% were re-using DDS in the Noncritical group, and 1.8% were re-using DDS in the Critical group.
2. Based on the type of clinic, the rate of re-use was higher in dental clinics, compared with dental hospitals.
3. The most re-use rate of supplies were Masks (64.6%), Prophylaxis cups (61.0%) and plastic saliva ejectors (30.0%).
These findings suggest that in order to ensure a safe environment within the dental clinic, DDS classifications must be clearly outlined in the dental infection control guidelines; moreover, additional studies are needed regarding the regulations for DDS re-use and disposal.

