Introduction
South Korea became an aged society in 2018 and is rapidly turning into a super-aged society. Following the rapid aging of the population, health care for the elderly has become an important issue, with the importance of oral health also emphasized [1]. In the elderly, oral health is related to mastication, swallowing, pronunciation, and esthetics. Additionally, it is closely related to nutrient intake and digestion, thereby playing an essential role in maintaining the overall health of the elderly [2]. Periodontal disease is an inflammatory condition affecting tooth-supporting tissues. Periodontal pocket deepening due to periodontal inflammation leads to alveolar bone loss, tooth mobility, and periodontal abscess formation. Failure to treat the disease can ultimately lead to tooth loss [3].
Compared to the incidence of other oral diseases, periodontal disease incidence is high in the elderly [4]. In the 2017 National Survey of Older Koreans, 89.5% of the elderly aged >65 years had more than one chronic disease, including periodontal disease [5]. Additionally, an oral health survey of the elderly aged >65 years showed low gingival elasticity and high periodontal disease morbidity among participants. Moreover, the elderly exhibited a poor capacity for oral hygiene maintenance and low interest in oral health education [6].
Risk factors for periodontal disease in the elderly include not only bacteria but also age, sex, socioeconomic factors, genetics, oral care habits, smoking, and systemic diseases [7]. Among them, smoking is one of the most important risk factors for periodontal disease [8]. Moreover, smoking causes impaired periodontal tissue response to periodontal treatment [9]; thus, it is expected to significantly influence periodontal disease development in the elderly.
Studies exploring the relationship between smoking and periodontal disease have reported smoking as a direct risk factor for poor oral health [10,11]; furthermore, tobacco smoke and the chemicals present in it have been associated with bacterial growth in the gingival tissue, leading to soft tissue destruction in the oral cavity [11,12]. In addition, many studies have shown that smoking increases the risk of periodontal disease [13,14]. Although several studies have evaluated the negative effects of smoking on periodontal disease, studies exploring the relationship between smoking history and periodontal disease among the elderly are lacking. Therefore, in this study, the relationship between smoking history and periodontal disease among the elderly in South Korea was assessed using data from the 7th Korea National Health and Nutrition Examination Survey (KNHANES; 2016–2018).
Methods
1. Research participants
Data from the 7th KNHANES (2016–2018) were used in this study. KNHANES is a nationwide survey assessing the health condition, health-related behavior, and food and nutrition intake status of South Koreans through health, medical, and nutrition surveys; it provides representative and reliable statistics at a national level. Additionally, KNHANES is used as basic data collection tool for devising health policies, including setting goals and evaluating National Health Plan, and for developing health promotion programs. Among a total of 24,269 individuals who participated in the 7th KNHANES, 3,426 elderly people aged >65 years underwent an oral examination. Among them, 2,703 elderly people who underwent periodontal examination as well as responded to items on smoking were included in this study, and their health survey and oral examination data were analyzed.
2. Research tools
1) Periodontal disease prevalence
Periodontal disease prevalence was evaluated using Community Periodontal Index (CPI). The index teeth included a maxillary right molar, maxillary central incisor, maxillary left molar, mandibular right molar, mandibular central incisor, and mandibular left molar. If a participant was observed to have a periodontal condition that would require interventions beyond oral prophylaxis, the participant was assessed to have periodontal disease.
2) Characteristics of the elderly in South Korea
The characteristics of the elderly included in this study were further divided into general, health-related, and oral health-related characteristics. General characteristics included sex (male or female), age (65-75 or ≥75 years), monthly household income (high, middle, or low), and employment status (employed or unemployed). Health-related characteristics included subjective health (good, average, or bad), current smoking status (current, former, or non-smoker), monthly alcohol consumption (less than or more than 1 drink per month in the past 1 year), aerobic physical activity (yes or no), average hours of sleep per week, and Patient Health Questionnaire-9 (PHQ-9) score. Oral health-related characteristics included subjective oral health (good, average, or bad), tooth brushing in the past day (yes or no), the number of oral health supplements used (0, 1, 2, or more than 4), oral examination in the past 1 year (yes or no), and unsatisfactory dental medical care (yes or no). Each variable was re-categorized to suit the purpose of this study.
3) Data analysis
The complex sample analysis method was used according to the complex sample design of the 7th KNHANES raw data. Cluster variables were determined by applying the survey group, and stratification variables were determined using strata. Weights for the variables were calculated by applying oral examination weights. Rao-Scott chi-square test was performed to assess periodontal disease status according to participant characteristics. Binary logistic regression analysis was performed to evaluate the relationship between smoking history and periodontal disease among the elderly. A p-value of <0.05 was considered statistically significant. All data were analyzed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp; Armonk, NY).
Results
1. Periodontal disease prevalence according to the participants’ general characteristics
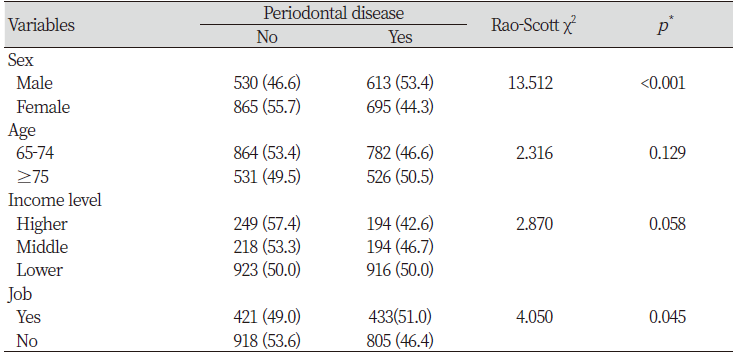
Of all participants, 53.4% men and 44.3% women required periodontal treatment; furthermore, 46.6% and 50.5% participants aged 65–74 years and ≥75 years, respectively, had periodontal disease. Moreover, 42.6%, 46.7%, and 50.0% of those with high, average, and low monthly household incomes, respectively, had periodontal disease. Additionally, 51.0% employed and 46.4% unemployed participants had periodontal disease. There were significant differences in periodontal disease prevalence according to sex and employment <Table 1>.
Table 1. Periodontal disease according to general characteristics of subjects Unit : N (Weight %)
|
|
*by complex sample chi-square test |
2. Periodontal disease prevalence according to health-related conditions
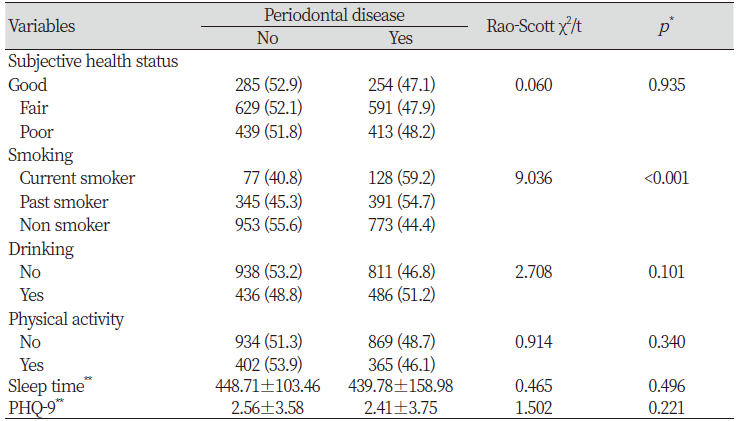
<Table 2> shows periodontal disease prevalence according to health-related characteristics of the elderly in South Korea; 47.1%, 47.9%, and 48.2% of the participants with good, average, and bad subjective health, respectively, had periodontal disease. The average hours of sleep per week was 439.78±158.98, and participants with a mean PHQ-9 (that evaluates depression) score of 2.41±3.75 were shown to have periodontal disease. Nevertheless, there was no significant difference in periodontal disease prevalence according to these health-related characteristics. However, there were significant differences in periodontal disease prevalence according to smoking history: 59.2% of current smokers, 54.7% of past smokers, and 44.4% of non-smokers had periodontal disease (p<0.001).
Table 2. Periodontal disease according to general health of subject Unit : N(%)
|
|
*by complex sample chi-square test or t-test, **Mean±SD |
3. Periodontal disease prevalence according to oral health-related characteristics
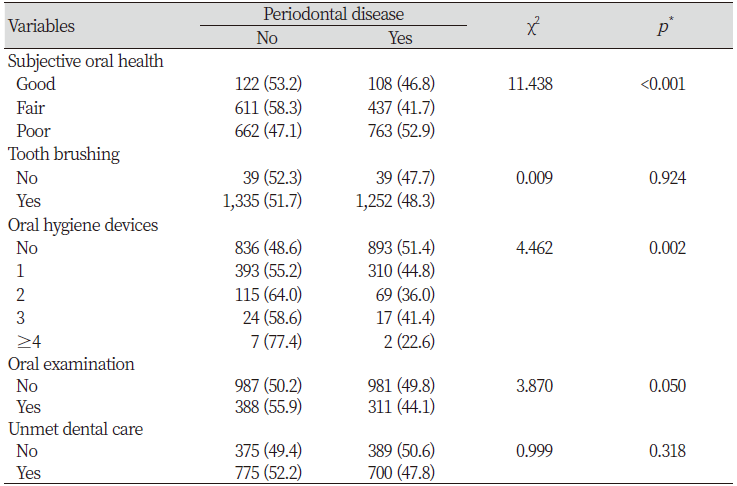
Among the participants, 46.8%, 41.7%, and 52.9% individuals with good, average, and bad subjective oral health, respectively, had periodontal disease. In addition, 51.4%, 44.8%, 36.0%, and 22.6% of those who used 0, 1, 2, and more than 4 oral health supplements, respectively, had periodontal disease. There were significant differences in periodontal disease prevalence according to the number of oral health supplements used <Table 3>.
Table 3. Periodontal disease according to general oral health of subjects Unit : N(%)
|
|
*by complex sample chi-square test |
4. Relationship between smoking history and periodontal disease in the elderly in South Korea
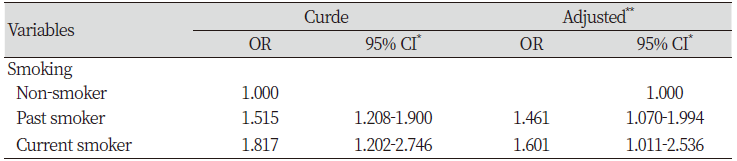
Variables with a p-value of <0.05 in univariate analysis were used as control variables for complex sample logistic regression analysis to investigate the relationship between smoking history and periodontal disease in the elderly in South Korea. The results showed that the odds of periodontal disease development were 1.461 times higher in past smokers (95% CI=1.070–1.994) and 1.601 times higher in current smokers (95% CI=1.011–2.536) than in lifetime nonsmokers <Table 4>.
Discussion
This study was conducted to assess the relationship between smoking history and periodontal disease, a chronic disorder, in elderly Koreans.
The results showed that the odds of periodontal disease development were higher in the past (OR=1.461; 95% CI=1.070–1.994) and current (OR=1.601; 95% CI=1.011–2.536) smokers than in lifetime non-smokers. These findings suggest that elderly current and past smokers are more vulnerable to periodontal disease development compared to elderly lifetime non-smokers. In a previous study on the relationship between smoking and periodontal disease in adults [15], periodontal disease prevalence was 1.75 and 1.82 times higher in past and current smokers, respectively, than in non-smokers. These findings are in agreement with our results.
Based on a previous study finding that smoking leads to increased periodontal pocket depth, loss of attached gingiva, tooth movement, and furcation lesions [8], it can be assumed that the elderly who smoke have increased vulnerability to risk factors for periodontal disease as the amount and duration of smoking is greater among them than among elderly past smokers and non-smokers. Additionally, smoking is closely related to environmental factors that can induce severe periodontitis [16]. Thus, periodontal disease prevalence is expected to be greater among elderly current smokers. In the elderly, aging-related degenerative changes in oral tissues lead to a decreased self-cleaning ability of the saliva and a decline in immune function in the oral cavity [17]. Therefore, it is necessary to prevent smoking, an environmental risk factor that can be improved, in the elderly.
Periodontal disease in the elderly is caused by chronic infection that remains undiagnosed and untreated for a prolonged period. Periodontal disease progresses rapidly after mid-thirties and may eventually lead to tooth extraction if not treated timely [18]. As most chronic diseases, including periodontal disease, are related to health behavior, it is fundamental for the elderly to practice and maintain health-promoting behaviors in order to maintain optimal health and function [19]. Therefore, it is necessary to continuously provide education on smoking cessation to smokers starting from the mid- to late 30s, the period during which periodontal disease progresses rapidly.
We observed that 51.4%, 44.8%, 36.0%, and 22.6% of the participants who used 0, 1, 2, and more than 4 oral health supplements (such as dental floss, interdental toothbrush, and tongue cleaner), respectively, had periodontal disease, suggesting that oral health supplement use significantly lowers periodontal disease prevalence. This finding is consistent with that of a previous study reporting that oral health status improved after interventions such as education on tooth brushing for self-care were continuously provided to the elderly in nursing homes [2]. These findings suggest that periodontal disease caused by degenerative changes in oral tissues of the elderly may be improved through oral health supplement use and education on tooth brushing.
Several limitations need to be considered in the interpretation of the present study findings. First, it was a cross-sectional study; therefore, the temporal relationship between smoking history and periodontal disease could not be evaluated. Moreover, smoking history was subjectively assessed using a questionnaire. Thus, the possibility of response bias cannot be excluded. However, despite these limitations, a complex sample design analysis was performed to determine the association between smoking history and periodontal disease in elderly Koreans using KNHANES data that are representative at a national level. Therefore, this study is meaningful as the results can be generalized to the entire elderly population in South Korea. However, future studies are warranted to evaluate the association between periodontal disease and the amount and duration of smoking.
Conclusions
This study was conducted to assess the association between smoking history and periodontal disease in elderly Koreans.
1. The odds of periodontal disease development were 1.461 times higher in past smokers than in non-smokers.
2. The odds of periodontal disease development were 1.601 times higher in current smokers than in non-smokers, suggesting that current and past smokers are more vulnerable to periodontal disease development compared to non-smokers.
These findings suggest that elderly smokers must actively participate in smoking cessation programs and interventions starting from middle age.

