Introduction
Periodontal disease first starts as an inflammation. The lack of proper management leads to symptoms such as gingival bleeding and recession, periodontal pocket formation, and destruction of alveolar bone, which subsequently cause tooth loss. This chronic disease is observed in adults and progresses in earnest after the age of 20 [1]. Approximately 85% of adults in Korea contracted periodontal disease, and the prevalence of peritonitis increases with age [2]. According to the Health Insurance Review and Assessment Service (HIRA) in 2019, ‘gingivitis and periodontal disease’ was ranked as the most common disease [3]. Periodontal disease is a bacterial infection of the periodontal tissue. Mature oral biofilms are calcified to plaques on the tooth surface and form on natural teeth or prosthesis. These plaques act as a local source of periodontal disease by causing mechanical stimulation to the gingiva and subsequent inflammation [4]. Therefore, scaling to remove oral biofilms and plaques is an essential procedure that determines the prevention and treatment of periodontal disease [5]. Local factors such as dental plaques and deposits that cause dental caries and periodontal disease may be removed [6] to improve the oral health.
Comprehensive dental hygiene care (CDHC) [assessment-dental hygiene diagnosis-planning-implementation-evaluation (re-evaluation after 4 weeks) + documentation] applied to scaling for more systematic and efficient management of periodontal disease is an evidence-based process to improve the oral health through oral disease prevention and treatment [7]. CDHC is an individually tailored professional dental hygiene process that reviews the oral health, finds potential problems, plans and executes customized prevention and treatment, and effectively manage the treatment through the evaluation of healing and results based on dental hygiene assessment [8]. As defined in social psychology, believe and behaviors are directly related to one another, and knowledge about an individual’s belief and attitude can accurately measure a given behavior [9]. The health belief model is the most influential and universally used model for explaining health-related behaviors [10]. The model has been previously used to describe the behaviors of people who believe oneself is healthy for the prevention and detection of disease in asymptomatic stage and its related factors [11]. For a quality life, it is necessary to increase not only health belief, but also oral health belief that can improve awareness and behavior of oral health. Therefore, the purpose of this study was to assess oral health belief and satisfaction after scaling experience with CDHC at dental hospitals and clinics and provide basic data on the necessity and clinical application of CDHC.
Methods
1. Participants and methods
This study was conducted from July 1, 2020 to September 20, 2020 with the approval of the 00 University Institutional Review Board (IRB) (IRB approval number:1041485-202005-HR-001-09). Those between the age of 20 and 65 who voluntarily agreed to this study and had experiences of scaling were conveniently extracted. Then, only those who understood the purpose of this study and provided a written consent form were asked to complete a self-administered questionnaire.
The minimum number of participants required for this study were calculated using G*power 3.1.9.4 program with an effect size of 0.15, significance of 0.05, and power of 0.85. A minimum number of 87 participants was required per group with a total of 174 participants. As a result, 190 participants were recruited, in consideration of 10% dropout rate. Among the retrieved questionnaires, six questionnaires were excluded for incomplete responses, and 184 questionnaires were included in the final analysis. A total of 92 participants were included in each of the two groups: scaling with CDHC (CDHC group) and scaling without CDHC (non-CDHC group).
2. Study tools
Oral health belief was evaluated using a tool developed by Kim [10], which was modified and supplemented for use in this study. The tool consisted of 25 items in total with 5 items for each of sensitivity, severity, benefit, importance, and disability. Each item was evaluated on a five-point scale from ‘strongly disagree’ for one point to ‘strongly agree’ for five points. For analysis, ‘strongly disagree’ and ‘disagree’ was converted into ‘disagree’, and ‘strongly agree’ and ‘agree’ were converted into ‘agree’. ‘Disagree’, ‘neutral’, and ‘agree’ were given a score of one, two, and three points, respectively for analysis. A higher score indicated a greater belief about sensitivity, severity, benefit, and importance, and a lower score indicated less disability.
Oral health behavior was evaluated using a tool used by Lee [11], which was modified and supplemented for use in this study. The tool consisted of seven items, including three items on the frequency, timing, and duration of brushing, two items on the use and type of oral hygiene supplements, one item on regular oral health checkups, and one item on regular scaling interval. Satisfaction was evaluated using a tool used by Hong et al. [12] and Han [13]. The tool was modified and consisted of eight items. Awareness of CDHC procedure was evaluated using a tool used by Moon et al. [14]. The tool was modified to reflect the dental clinical settings in Korea, and items on periodontal examination during CDHC process were re-written in simpler terms to enhance the understanding of the participants. The tool consisted of 10 items in total. Cronbach’s α excluding general characteristics, was 0.749 for oral health belief and 0.890 for satisfaction.
3. Statistical analysis
Data were analyzed using SPSS for Window version 22.0 (IBM Co, Armonk, NY, USA), and all statistical significance (α) was set to 0.05. Chi-square test was conducted to compare oral health behaviors between the groups who underwent scaling with or without CDHC. Independent sample t-test and one-way ANOVA were conducted to compare oral health belief and satisfaction according to general characteristics and oral health behaviors. Scheffé test was conducted for post-hoc analysis. Independent sample t-test was conducted to compare oral health belief and satisfaction according to the awareness of CDHC. Lastly, Pearson’s correlation analysis was performed on the relationship between satisfaction and sub-factors of oral health belief in the CDHC group.
Results
1. Oral health behavior of CDHC and non-CDHC groups
Approximately 92.4% of CDHC group and 70.7% of non-CDHC group used oral care products other than toothbrush and toothpaste (p<0.001). In the CDHC group, 67.4% visited the dental hygienist on a regular basis for oral care. On the other hand, only 33.7% of the non-CDHC group regularly visited the dental hygienist for oral care (p<0.001). In the CDHC group, 38.0%, 34.8%, 16.3%, and 10.9% underwent scaling every 12 months, six months, three months, and other, respectively. In the non-CDHC group, 60.9%, 12.0%, 3.3%, and 23.9% received scaling every 12 months, six months, three months, and other, respectively (p<0.001) <Table 1>.
|
Table 1. Oral health behavior of CDHC and non-CDHC groups Unit:(N%) 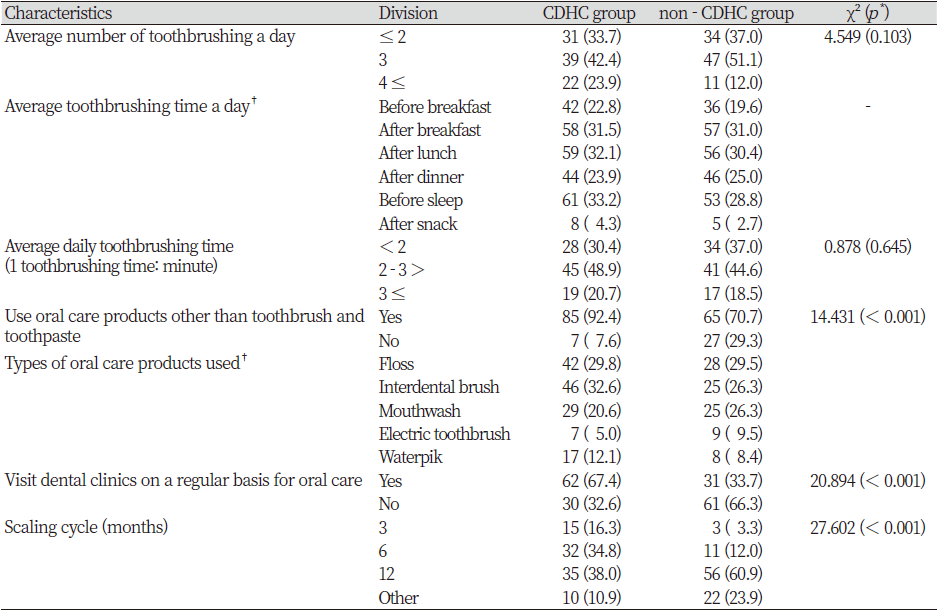
|
|
*by chi-square test †multiple responses |
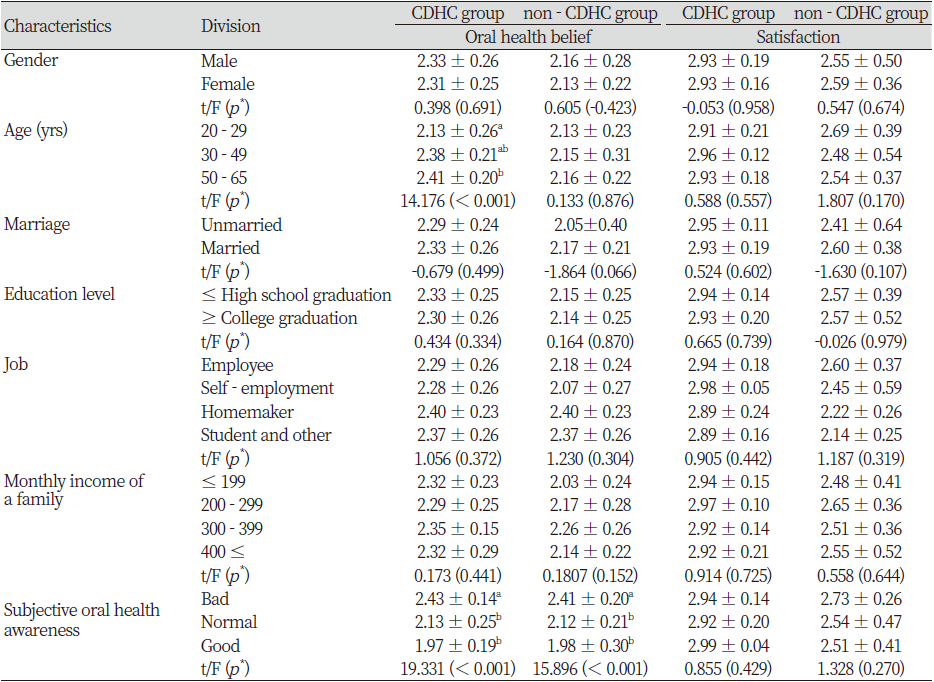
2. Oral health belief and satisfaction according to general characteristics of CDHC and non-CDHC groups
In the CDHC group, those between the age of 50-65 had the highest score for oral health belief at 2.41 points. Post-hoc analysis showed that those between the age of 50-65 had a significantly greater score for oral health belief than those between the age of 20-29 (p<0.001). Oral health belief was high at 2.43 points as subjective oral health awareness was ‘bad’. Post-hoc analysis showed that the oral health belief of those with ‘bad’ subjective oral health awareness were significantly higher than that of those with ‘normal’ and ‘good’ subjective oral health awareness (p<0.001). In the non-CDHC group, oral heath belief was high at 2.41 points as subjective oral health awareness was ‘bad’. The oral health belief of those with ‘bad’ subjective oral health awareness were significantly higher than that of those with ‘normal’ and ‘good’ subjective oral health awareness (p<0.001) <Table 2>.
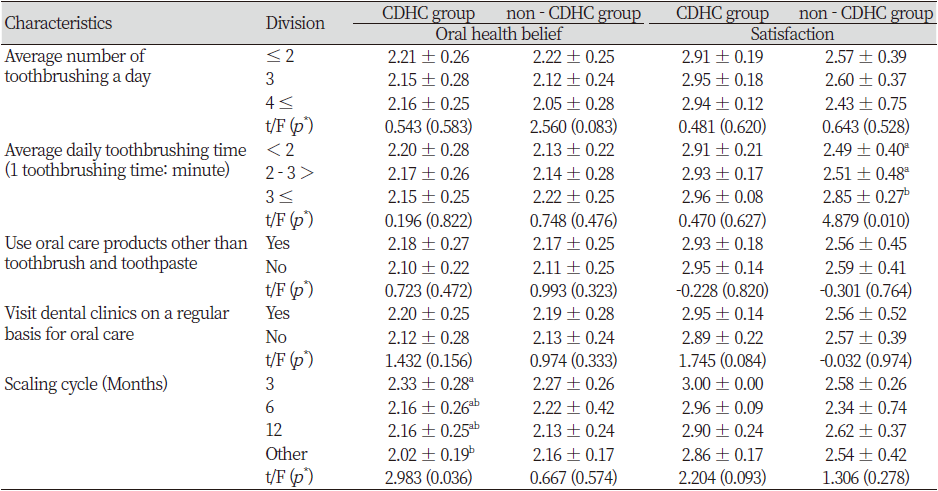
3. Oral health belief and satisfaction according to oral health behaviors in CDHC and non-CDHC groups
In the CDHC group, the oral health belief was highest in those who underwent scaling ‘every three months’ at 2.33 points. The oral heal belief of those undergoing scaling ‘every three months’ was significantly higher than that of those undergoing scaling ‘other’ (p<0.05).
In the non-CDHC group, the oral health belief was highest in those who brushed their teeth for ‘more than three minutes’ on average per time at 2.85 points. The oral health belief of those who brushed teeth for ‘more than three minutes’ was significantly higher than that of those brushing for ‘less than two minutes’ and ‘two to three minutes’ (p<0.05) <Table 3>.
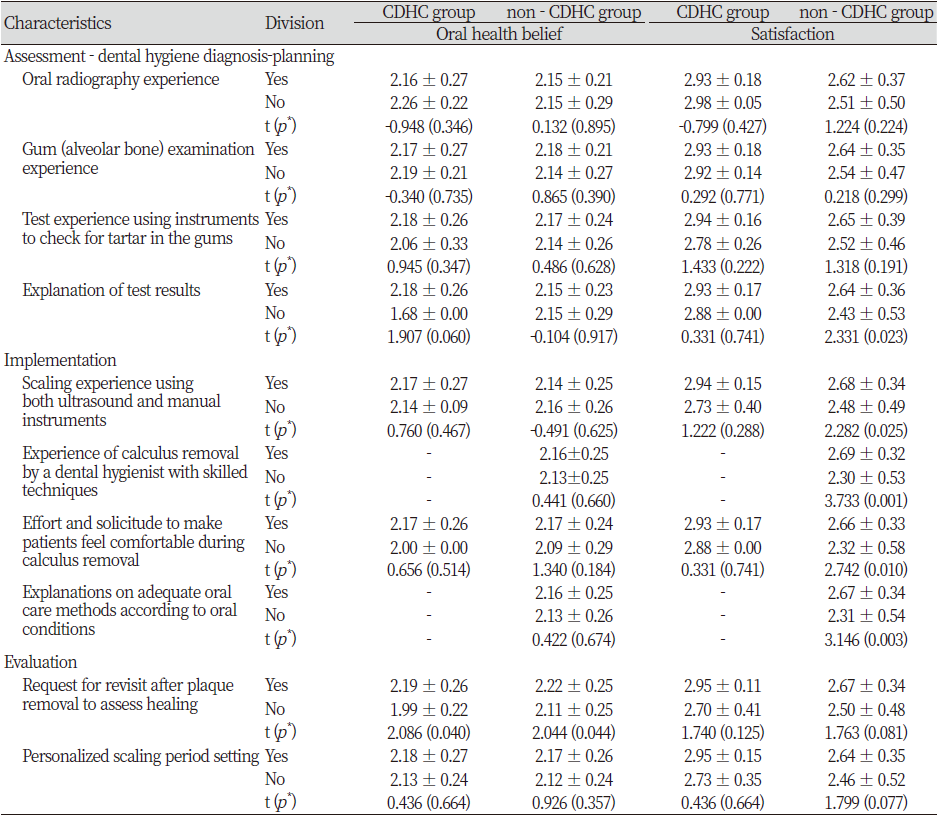
4. Oral health belief and satisfaction according to the awareness of CDHC process in CDHC and non-CDHC groups
Oral health belief according to the awareness of CDHC process was analyzed. The request for revisit after plaque removal to assess healing was high in both CDHC (2.19, p<0.05) and non-CDHC (2.22, p<0.05) groups. In the non-CDHC group, satisfaction increased with explanation of test results (2.64, p<0.05), scaling experience using both ultrasound and manual instruments(2.68, p<0.05), proficient experience of the dental hygienist with skilled techniques for calculus removal (2.69, p<0.05), effort and solicitude to make patients feel comfortable during calculus removal (2.66, p<0.05), and experiences of receiving explanations on adequate oral care methods according to oral conditions (2.67, p<0.01) <Table 4>.
5. Correlation between sub-factors of oral health belief and satisfaction in CDHC group
Correlation between sub-factors of oral health belief and satisfaction was evaluated in CDHC group. Satisfaction was positively correlated with benefit (r=0.291, p<0.01) and importance (r=0.224, p<0.05) <Table 5>.

Discussion
This study was conducted to assess differences in oral health belief and satisfaction according to scaling experiences with CDHC and provide basic on the application of CDHC. In the CDHC group, 33.7%, 42.4%, and 23.9% brushed teeth ‘less than two times’, ‘three times’, and ‘more than four times’ a day, respectively. In the non-CDHC group, 37.0%, 51.1%, and 12.0% brushed teeth ‘less than two times’, ‘three times’, and ‘more than four times’ a day, respectively. In both groups, the highest proportion of participants brushed teeth ‘three times a day’. In a previous study by Kim [15] using the 2015 Korea National Health and Nutrition Examination Survey (KNHANES), 48.3%, 35.8%, and 15.8% brushed teeth ‘less than two times’, ‘three times’, and ‘more than four times’ a day. Compared to these findings, the participants in our study showed improved behavior of brushing. Additionally, in a study of patients with gingivitis and periodontitis who visited dental hospitals or clinics, Moon et al. [16] observed that the greatest proportion of both patient groups with gingivitis and periodontitis brushed teeth ‘three times’ a day. This finding is in agreement with that of our study. Herein, we observed that 92.4% of the CDHC group and 70.7% of the non-CDHC group used oral care products other than toothbrush and toothpaste. The most common types of oral care products included ‘interdental brush’ (50.0%), ‘floss’ (45.7%), and ‘mouthwash’ (31.5%) in the CDHC group and ‘floss’ (30.4%), ‘interdental brush’ (27.2%), and ‘mouthwash’ (27.2%) in the non-CDHC group. Kim [15] reported that 23.3%, 22.7%, and 19.9% of patients used ‘floss’, ‘mouthwash’, and ‘interdental brush’, respectively. The rate of oral care product use was higher in our study than that in the study by Kim. This may be attributed to the motivation and education for self-management by dental hygienists as the participants of our study received scaling in dental clinics or hospitals.
In the CDHC group, the proportion of those who visited dental clinics on a regular basis was approximately two times higher than that in the non-CDHC group. It is thought at the oral health education or customized scaling interval during CDHC process by dental hygienists may have had effects. The most common scaling interval was ‘12 months’ (38.0%) and ‘six months’ (34.8%) in the CDHC group and ‘12 months’ (60.9%) and ‘other’ (23.9%) in the non-CDHC group. In the non-CDHC group, majority of the participants received scaling every 12 months, and this may be due to the coverage of scaling by the national health insurance system. Thus, to improve the oral health of a patient, a dental hygienist needs to set up a customized scaling cycle through re-evaluation after scaling.
Oral health belief was significantly high in CDHC group participants between the age of 50 and 65. Consistent with our finding, Park [17] previously reported that oral health belief, oral health practice, and oral health-related quality of life were significantly higher in those between the age of 40 and 60. Middle-aged and elderly people suffer from functional loss of teeth and are aware of health risk factors such as poor oral care, stress, drinking, and smoking [18]. This may have contributed to the high oral health belief in those between the age of 50 and 60 in our study. In the CDHC group, the participants respond ‘yes’ (100.0%) to the item on ‘experience of calculus removal by a dental hygienist with skilled techniques’ and ‘explanations on adequate oral care methods according to oral conditions’. Additionally, our results showed that the satisfaction was higher in all items in the CDHC group than in the non-CDHC group. This suggested that the awareness of CDHC process in the participants may have affected satisfaction with scaling experiences.
Herein, we observed that in the CDHC group, benefit and importance, which are sub-factors of oral health belief, were positively correlated with satisfaction. This finding is in agreement with the results of a study of adults who visited dental clinics by Choi and Park [19]. In that study, sensitivity was positively correlated with severity and importance. Severity was positively correlated with benefit and importance. Additionally, benefit was significantly correlated with importance. Based on our findings that higher belief on the benefit and importance of oral health is associated with higher satisfaction of scaling experiences, educational competency of dental hygienists must be improved. This study demonstrated that CDHC during scaling and non-surgical periodontal treatment may have positive effects of increasing oral health belief and satisfaction of patients and that scaling with CDHC by dental hygienists may contribute to the management of oral health. Therefore, CHDC should be more actively used in clinical practice to improve the expertise of dental hygienists and increase the belief and satisfaction of patients in oral health. However, several limitations must be considered in the interpretation of this study’s findings. Patients who underwent scaling at dental hospitals and clinics were extracted through a convenience sample method. Moreover, some of the processes in the CDHC and non-CDHC groups were identical, limiting complete distinguishment of the two groups. Follow-up studies would need to develop a research tool that can analyze in detail the satisfaction of patients with scaling experiences and conduct an in-depth analysis of the effects of CDHC.
Conclusions
In this study, oral health belief and satisfaction in the CDHC and non-CDHC groups were analyzed using the oral health belief model, and basic data for the clinical use of CDHC were obtained. Data were collected from 184 participants, and the following conclusions were obtained.
1. Oral health behavior in the CDHC group was as follows: 92.4% used oral care products other than toothbrush and toothpaste (p<0.001), and 67.4% visited dental clinics on a regular basis for oral care (p<0.001).
2. In the CDHC group, oral health belief was the highest with 2.41 points in those between the age of 50-65. Oral health belief of those between the age of 50-65 was significantly different from that of those between the age of 20-29 (p<0.001).
3. In the CDHC group, oral health belief according to oral health behaviors was the highest in those who underwent scaling every ‘three months’ (p<0.05).
4. In the CDHC group, benefit (p<0.01) and importance (p<0.05), which are sub-factors of oral health belief, were positively correlated with satisfaction.
These results showed that CDHC had positive effects on increasing the oral health belief and satisfaction of scaling experience. Thus, CDHC must be used more actively in clinical practice to increase oral health belief and satisfaction of patients undergoing scaling.


