Introduction
As the health paradigm has changed from treating diseases to preventing diseases and maintaining and promoting health, health promotion has become a social concern not only for health care professionals but also for general adults. Accordingly, the need for oral health management is emphasized as oral health is also part of overall health and has a significant influence on life [1,2]. Since the loss of teeth or oral tissue due to oral diseases cannot be regenerated even if it can be replaced, prevention and care should be taken to prevent oral disease. Therefore, it is crucial not only to visit a dental clinic for treatment but also to perform oral health behavior for oral health management. In addition, it is necessary to identify measures that can lead to the ability to easily obtain and utilize information related to oral health and factors influencing oral health behavior.
Along with the increase in internet use, the digital gap for individual internet use decreases, and the internet is playing the role of a medium for health information [3]. The term, e-health, which has the concept of utilizing information and communication technology in the medical or health field, has emerged. The World Health Organization (WHO) defined it as the “interchange of health information using new communication science and technology” [4]. e-health has the advantage of improving the efficiency and accessibility of medical services. People who have difficulty receiving medical services can obtain health information on the internet and receive help in oral health management [5]. ‘Healthy people 2030’ of the U.S. Department of Health and Human Services emphasized patient-centered health care and focused on health communication and health information technology to help patients explore and share health information for their health management and promote health [6].
e-health literacy refers to the ability to search, understand, evaluate, and apply health information about one’s health-related issues online [7]. The previous study related to e-health literacy in Korea has shown that e-health literacy affects health promotion behavior [8]. Low e-health literacy may lead to the inability to effectively use internet health information, lack of information, distortion of information, and health imbalances and medical disparity problems. Thus, it is necessary to improve the level of e-health literacy in individuals who can judge and utilize correct information.
The oral health knowledge level of individuals will be helpful in oral health behavior for self-oral care, emergencies occurring at home, and dental treatment, and if the level of knowledge related to oral health increases due to the acquisition of oral health knowledge, the attitude of oral health changes and correct oral health behavior can be performed, which will have a positive effect on oral health [9]. Since adults have time and space limitations to acquire oral health knowledge, it is challenging to learn oral health knowledge through oral health education organized by dental clinics or public institutions. Thus, acquiring oral health knowledge from the internet will be very useful.
In line with the development of medical technology and internet information technology, many studies have been conducted on e-health literacy in the medical field, but there are no studies on e-health literacy in the oral health care field. Efforts should be made in various ways to effectively use e-health to receive and utilize high-quality oral health information.
This study aims to identify new variables that can promote oral health behavior in adults by exploring the level of e-health literacy, oral health knowledge, and oral health behavior in adults and provide fundamental data for effective strategy development.
Methods
1. Study subject
This study was conducted with the approval of the Institutional Review Board of 00 University (IRB No: NSU-202105-004). From June 22, 2021, to August 1, 2021, study subjects were recruited through SNS (Social Network Service) for adult males and females aged 19 years or older using a convenience sampling method. The subjects were adults who understood the explanation and purpose of the study and consented to the study through the online recruitment notice. The survey was conducted online using NaverForm, a web-based questionnaire. A total of 350 subjects were included based on the evidence that 300 or more subjects are appropriate for the number of study subjects [10]. Of the 350 questionnaires, a total of 312 were used as the final analysis data, excluding 38 questionnaires that were not filled out faithfully.
2. Study tool
The study tool consisted of 77 questions, including 15 general characteristics items, 31 e-health literacy items, 18 oral health knowledge items, and 13 oral health behavior items.
1) General characteristics
It consisted of socio-demographic characteristics, oral health-related characteristics, and internet-related characteristics.
2) e-health literacy
e-health literacy refers to the ability to search, understand, evaluate, and apply health information on one’s health-related issues online [7]. It consists of functional e-health literacy, which is the ability to read, understand, and write health information; communicative e-health literacy that finds and applies health information to communication; and critical e-health that analyzes and interprets health information to use it for health management or health problems [11]. This study used the e-health literacy tool developed by Lee [11], and the questions about general health were modified to suit oral health. Each item is measured on a 5-point Likert scale, ranging from ‘strongly agree’ to ‘not at all’ from 5 to 1, with higher scores indicating higher e-health literacy. At the time of tool development, communicative e-health literacy was Cronbach’s α=0.920, critical e-health literacy was Cronbach’s α=0.927, and functional e-health literacy was Cronbach’s α=0.903. Reliability in this study was Cronbach’s α=0.877 for communicative e-health literacy, Cronbach’s α=0.933 for critical e-health literacy, and Cronbach’s α=0.900 for functional e-health literacy.
3) Oral health knowledge
The questionnaire used by Lee [9] was modified and used for oral health knowledge, and it consisted of contents related to teeth, periodontal, and oral hygiene products. The total was calculated by reclassifying each item into the correct answer (1) and incorrect answer (0), and the higher the score, the higher the oral health knowledge. There are 18 items, and if all the items are correct, it will be 18 points. In this study, the reliability was Cronbach’s α=0.872.
4) Oral health behavior
For oral health behavior, the questionnaire used by Lee [9] was modified and used, and it consisted of dietary habits, use of oral hygiene products, regular dental checkups, and smoking. Each item is measured on a 5-point Likert scale, ranging from 5 points to ‘always’ to 1 point to ‘never,’ and the higher the average value, the higher the level of oral health behavior. In this study, the reliability was Cronbach’s α=0.746.
3. Data analysis
The IBM SPSS Statistics 23.0 program was used for data analysis, and the significance level was set as α=0.05. Independent sample t-test and one-way ANOVA were performed for differences in oral health behavior depending on the general characteristics of study subjects, and a post-hoc test was performed using the Scheffé test. Hierarchical regression analysis was performed to determine the factors affecting oral health behavior.
Results
1. The average of e-health literacy, oral health knowledge, and oral health behavior of the study subjects
The average e-health literacy of the study subjects was 3.50. Communicative e-health literacy was 3.56, critical e-health literacy was 3.42, and functional e-health literacy was 3.54. Oral health knowledge was found to be an average of 12.53 out of a total of 18 points when the correct and incorrect answers were reclassified and summed. The average oral health behavior was 3.38 <Table 1>.
|
Table 1. e-health literacy, oral health knowledge, oral health behavior (N=312) 
|
|
*The range of oral health knowledge score is 0 to 18 points. |
2. Differences in oral health behaviors according to general characteristics
1) Oral health behavior according to socio-demographic characteristics
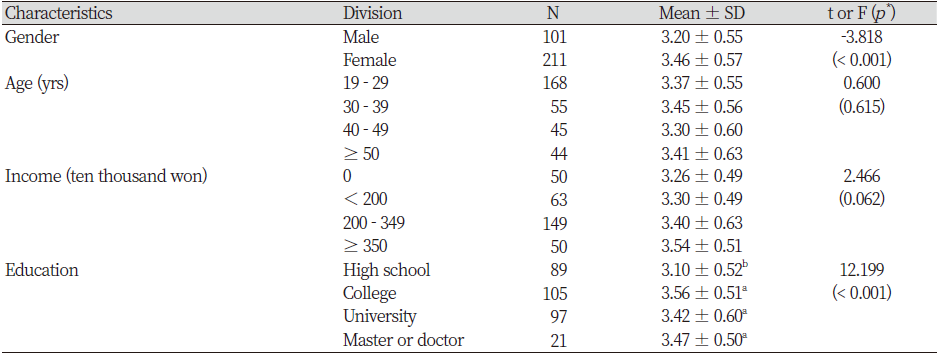
Among general characteristics, oral health behavior according to socio-demographic characteristics was found to have statistically significant differences depending on gender (p<0.001) and educational background (p<0.001). In terms of gender, females had higher average scores for oral health behavior than males, and Scheffé post-hoc analysis showed ‘college graduate’, ‘4-year university graduate’, and ‘graduate school or above’ had higher average scores than ‘high school graduate’ <Table 2>.
2) Oral health behavior according to oral health-related characteristics
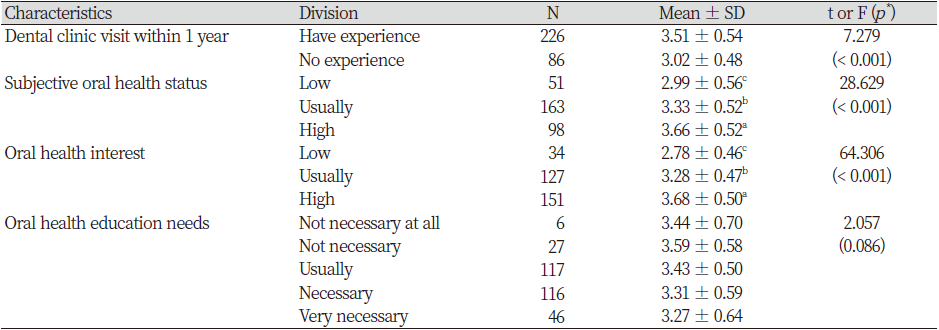
Among the general characteristics, oral health behavior according to oral health-related characteristics was found to have statistically significant differences depending on the experience of visiting a dental clinic within one year (p<0.001), subjective oral health status (p<0.001), and oral health interest (p<0.001). The average score for oral health behavior was higher in those who have experience visiting a dental clinic within one year than in those who did not have experience. In addition, Scheffé post-hoc analysis showed ‘normal’ of subjective oral health status and oral health interest was higher than ‘low’, and ‘high’ was higher than ‘normal’ <Table 3>.
3) Oral health behavior according to internet-related characteristics
Among general characteristics, oral health behaviors according to internet-related characteristics had statistically significant differences depending on the frequency of internet use for oral-related (p<0.001) and the reliability of internet oral health information (p<0.001). The average score for oral health behavior was higher in subjects who used the internet for oral-related more than three times a month than those who used the internet for oral-related less than three times a month, and Scheffé post-hoc analysis showed that the reliability of internet oral health information was higher in ‘normal’ and ‘high’ than in ‘low’ <Table 4>.

3. Factors affecting oral health behavior
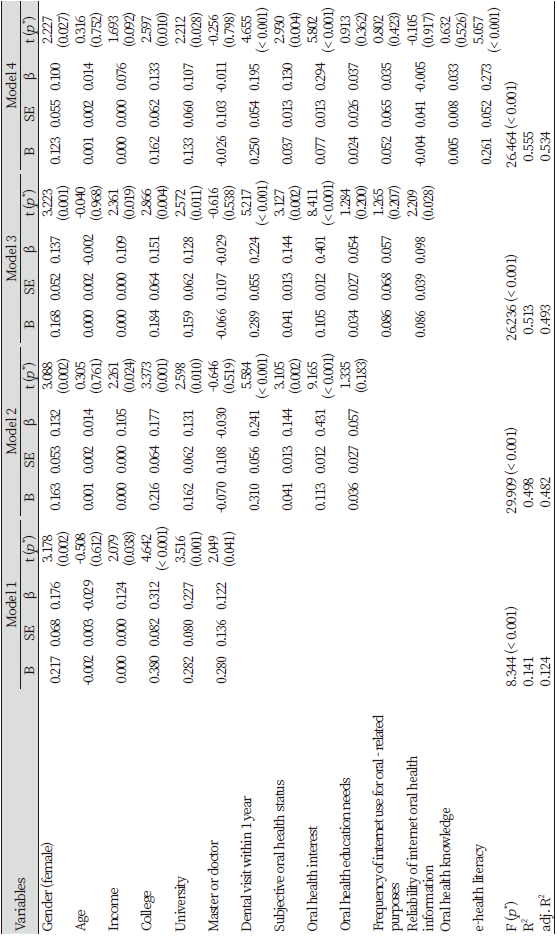
To investigate whether e-health literacy and oral health knowledge affect oral health behavior even after controlling general characteristic variables, a hierarchical regression analysis was performed by dividing socio-demographic characteristics, oral health-related characteristics, internet-related characteristics, and independent variables, e-health literacy and oral health knowledge, into four stages. Hierarchical regression analysis was performed by dividing knowledge into four stages. As a result of the analysis, F values were all significant with F=8.344 in Model 1 (p<0.001), F=29.909 in Model 2 (p<0.001), F=26.236 in Model 3 (p<0.001), and F=26.464 in Model 4 (p<0.001). In addition, the tolerance from Model 1 to Model 4 was 0.514. ~ 0.914, and the variance inflation factor was 1.094 ~ 1.946, showing no multicollinearity problem.
Model 1 identified the effect on oral health behavior by inputting socio-demographic characteristics as a control variable. The explanatory power of Model 1 was 0.124. In Model 1, gender had a significant effect on females than males (β=0.176, p=0.002), income (β=0.124, p=0.038) had a significant effect, and the educational background had a significant impact on college graduate (β=0.312, p<0.001), 4-year university graduate (β=0.227, p=0.001), and graduate school graduate (β=0.122, p=0.041) rather than high school graduate. In Model 2, oral health-related characteristics were additionally added as a control variable, and the explanatory power was 0.482, an increase of 35.8% compared to Model 1. Experience visiting a dental clinic within one year (β=0.241, p<0.001), subjective oral health status (β=0.144, p=0.002) and oral health interest (β=0.431, p<0.001) had a significant effect in Model 2. In Model 3, internet-related characteristics were additionally added as a control variable, and the explanatory power was 0.493, an increase of 1.1% compared to Model 2. The reliability of internet oral health information in Model 3 (β=0.098, p=0.028) had a significant effect. Model 4 added the independent variables, e-health literacy and oral health knowledge, to investigate whether e-health literacy and oral health knowledge affect oral health behavior even after controlling exogenous variables. The explanatory power was adj.R2 =0.534, an increase of 4.1% compared to model 3. Gender, educational background, experience visiting a dental clinic within one year, subjective oral health status, and e-health literacy were found to affect. It was found that the higher the e-health literacy (β=0.273, p<0.001), the statistically significant increase in oral health behavior, but oral health knowledge had no significant effect <Table 5>.
Discussion
This study was conducted to identify the relationship between e-health literacy, oral health knowledge, and oral health behavior in adults and determine the factors affecting oral health behavior.
In the differences in oral health behavior, there were significant differences in gender and education background among socio-demographic characteristics, experience visiting a dental clinic within one year, subjective oral health status and oral health interest showed significant differences among oral health-related characteristics, and there were significant differences in the frequency of internet use for oral-related and the reliability of internet oral health information among internet-related characteristics. In terms of gender, ‘females’ showed higher oral health behavior. It was similar to the study results of Kim [12] and Lee and Kim [13], which found that females had higher oral health-related behavioral scores than males. In terms of educational background, oral health behavior was higher among those who graduated from college or above than those who graduated from high school. It was similar to Kim [14] that the higher the level of education, the higher the number of brushing and dental clinic visits. Since colleges and four-year universities have departments related to health and medicine, it is believed that oral health behavior was higher than those who graduated high school.
In terms of oral health-related characteristics, oral health behavior was higher in subjects who had visited a dental clinic within one year. It is similar to the study results by Choi et al. [15] that subjects who regularly visit a dental clinic continued to have high experience in oral health management. Since adults’ visits to a dental clinic for oral examination are a willingness and independent choice to improve their oral health, it is thought that they show a more active attitude in performing oral health behavior. Moreover, it is believed to affect oral health behavior because it manages their oral health by visiting a dental clinic to prevent and treat oral diseases. The higher the subjective oral health status, the higher the oral health interest, and the higher the reliability of internet oral health information, the higher the level of oral health behavior. It is considered to have high confidence in subjective oral health status and a high level of oral health behavior because people with a high interest in oral health accept information and knowledge related to oral health actively and appropriately utilize information to apply it to oral care. In a study by Lee et al. [16], analyzing the quality of life depending on the subjective oral health status, it was found that the subjectively perceived oral health problems negatively affected the quality of life. The high subjective oral health status is believed to be based on individual confidence in oral health status and self-efficacy in oral management, and it was similar to the result that subjective oral health status affects oral health behavior in the study by Ahn and Lee [17]. Therefore, it also affects oral health behavior to maintain a healthy state.
Hierarchical regression analysis by controlling for general characteristic variables showed that e-health literacy was a factor influencing oral health behavior, similar to Nam’s study [18], in which e-health literacy affects health promotion behavior. Although the tools are different, in studies by Park [19] and Song and Shin [20], e-healthy literacy is a variable that explains the continuity of health behavior, the lower the age of the elderly and the higher the level of education, the higher the e-health literacy, which was similar to the result showing a positive correlation with health behavior. However, oral health knowledge was found to have no significant effect on health behavior, similar to the result that oral health knowledge did not affect oral health behavior in a study by Ahn and Lee [17].
This study identified e-health literacy as an essential factor influencing oral health behavior. To increase oral health behavior in adults and maintain and promote oral health through correct oral health behavior, it is necessary to improve e-health literacy competency to search and judge high-quality oral health information on the internet. This study is significant in that it was identified that e-health literacy in adults is a factor influencing oral health behavior. One of the limitations of this study is that it is difficult to directly compare and analyze the e-health literacy tools and concepts used with other studies as there are no previous studies related to oral health. In addition, it is difficult to generalize to all adults because the number of samples for male and female adults is not the same by using a convenience extraction method. As this study showed differences in oral health behavior depending on gender, more factors related to e-health literacy should be determined through follow-up studies without gender ratio differences and studies involving various subjects using the internet for use in dentistry and dental hygiene fields. Furthermore, follow-up studies are needed to measure e-oral health literacy suitable for a dental field by developing an e-oral health literacy tool and understand the effect on oral health behavior through investigations on e-health literacy related to oral health.
Conclusions
This study aims to seek measures to help oral health behavior by identifying the level of e-health literacy, oral health knowledge, and oral health behavior in adults and analyzing factors affecting oral health behavior. Three hundred fifty adults participate in the survey, and a total of 312 data were analyzed to obtain the following conclusions.
1. The overall average of e-health literacy was 3.50, followed by communicative e-health literacy of 3.56, functional e-health literacy of 3.54, and critical e-health literacy of 3.42 as sub-factors. The overall average of oral health knowledge was 12.53, and oral health behavior was 3.38.
2. Oral health behaviors according to general characteristics showed significant differences in gender, educational background, dental clinic visit experience within one year, subjective oral health status, oral health interest, frequency of internet use for oral-related, and reliability of internet oral health information.
3. After controlling for general characteristics, e-health literacy was found to affect oral health behavior.
Therefore, it is thought that measures are needed to improve e-oral health literacy so that there is no discriminated group in acquiring information by identifying the level of e-oral health literacy related to oral health. Moreover, it is necessary to seek measures to promote oral health behavior by utilizing e-oral health literacy.



