
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Soo-Min Kim![]() , Eun-Bi Cho
, Eun-Bi Cho![]() , Sun-Young Han
, Sun-Young Han![]()
Department of Dental Hygiene, College of Software and Digital Healthcare Convergence, Yonsei University
Correspondence to Sun-Young Han, Department of Dental Hygiene, College of Software and Digital Healthcare Convergence, Yonsei University, 1 Yonseidae-gil, Wonju-si, Gangwon-do, 26493, Korea. Tel: +82-33-760-5562, Fax: +82-33-760-5575, E-mail: syhan0724@yonsei.ac.kr
Volume 24, Number 5, Pages 373-84, October 2024.
J Korean Soc Dent Hyg 2024;24(5):373-84. https://doi.org/10.13065/jksdh.20240502
Received on September 10, 2024 , Revised on September 30, 2024, Accepted on October 01, 2024, Published on October 30, 2024.
Copyright © 2024 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0)

Objectives: This scoping review aimed to identify and analyze intervention strategies and assessment methods for oral hygiene management (OHM) and oral function management (OFM) in patients with stroke admitted to general wards, with the goal of providing directions for future research. Methods: We conducted a comprehensive literature search on studies published over the past 10 years across databases, including Cochrane, Embase, Medline, PubMed, and ProQuest. A total of 18 studies met the inclusion and exclusion criteria. Results: In the OHM studies (N=7), oral hygiene care was primarily provided by nurses, dental assistants, and nursing care aides. Oral hygiene was assessed using plaque and gingival bleeding indices with products such as electronic toothbrushes and mouth rinses. In the OFM studies (N=11), care was provided by speech-language pathologists, occupational therapists, and dental hygienists. Assessment tools included the Functional Oral Intake Scale, the PenetrationAspiration Scale, and Video Fluoroscopic Swallowing Studies. Conclusions: Improving the oral health of patients with stroke requires both hygiene and functional management. Therefore, it is necessary to develop a method that provides specialized oral care tailored to the hospitalization environment and the specific conditions of patients with stroke.
Inpatient, Oral function, Oral hygiene, Scoping review, Stroke
뇌졸중 환자는 신체 마비 등 후유증으로 일상생활에 어려움을 겪으며, 삼킴장애는 29-81%가 경험하고 흡인성 폐렴은 가장 흔히 나타나는 합병증으로 약 12%를 차지하며, 사망률은 5%에 달한다[1,2]. 뇌졸중 환자의 신체 마비는 구강위생관리를 어렵게 하여 치주질환을 악화시키고[3,4], 삼킴장애가 있는 경우에는 타액 및 볼루스 제거력이 떨어지면서 구강 내 미생물의 군집화를 높이기 때문에 흡인성 폐렴의 발생률이 높아진다[5,6].
뇌졸중 환자는 급성기 또는 재활치료 중에 구강위생관리를 소홀히 하는 경향이 있는데, 의료인과 보호자의 인식 부족이 가장 큰 원인으로 지목되었고[7], 다른 연구에서는 뇌졸중 환자에 대한 의료인의 교육 부족과 장비 및 재료 부족[8]이 원인으로 보고되기도 하였다[9]. 구강위생관리의 제공자는 주로 간병인, 간호사, 간호조무사, 치과조무사 이었고, 수행 행위로는 칫솔질과 치실을 포함한 구강위생관리가 가장 많았다[10]. 입원환자는 신체거동 상태와 구강기능 및 입원환경 등에 따라 개인화된 구강위생관리를 계획하고 수행하는 것이 필요하며, 이를 위해서는 치의학 및 치위생학적 전문 지식이 요구된다. 그러나 주 진료를 담당하는 재활의학과 일반의학에서는 치과와의 협진이 잘 이루어지지 않을 수 있고, 담당 의료진의 구강건강관리에 관한 인식이 부족할 수 있다. 또한 치과에서는 내원하는 외래환자의 구강질환 진단을 주로 치료하기 때문에 입원환자의 구강 문제를 해결하기 어려운 실정이다[11]. 최근 치과위생사에 의한 구강관리의 효과를 보고한 연구에 따르면, 요양시설 노인에게 전문적인 구강위생관리를 제공하여 치태 지수가 감소하고, 구강기능 훈련을 제공해 구강기능을 향상시키는데 기여하였다[12]. 전문적인 구강관리는 환자의 병원 감염과 인공호흡기 관련 폐렴 발병 위험을 감소시킬 수 있었는데[13], 그 예로 뇌혈관 질환자에게 치과위생사가 칫솔질과 구강보건교육을 제공했을 때 환자의 구강건강상태가 향상되었으며[14], 뇌졸중 및 고관절 골절 입원환자 병동에서 치과위생사가 전담하여 구강관리를 한 연구에서는 식품 섭취 수준 척도(FILS; Food Intake Level Scale), 기능적 독립성 척도(FIM; Functional Independence Measure), 퇴원 시 영양 상태(MNA-SF; Mini Nutritional Assessment Short-Form)가 개선되었을 뿐만 아니라 가정으로의 퇴원율이 높아졌다[15]. 즉, 전문가에 의한 중재는 입원환자의 구강건강 회복에 기여할 수 있음을 의미한다. 연하장애에 의한 합병증인 흡인성 폐렴 및 영양실조는 노인의 가장 높은 사망 원인 중 하나[16]로 연하장애를 겪고 있는 뇌졸중 환자의 경우 정상적 삼킴이 가능한 사람보다 사망할 위험이 약 8.5배가 높아 중재 프로그램이 더욱 필요하다[17]. 8주간 연하 훈련 프로그램을 요양시설에 거주하는 뇌졸중 노인에게 적용하였을 때 삼킴문제가 약 23% 감소하는 효과가 있었다[18].
그러므로 뇌졸중 환자의 건강을 위해 개인마다 다른 신체 활동 범위와 구강근육의 마비 수준 등을 고려하여 전문성을 갖춘 치과위생사가 구강위생관리를 비롯해 구강기능을 향상시킬 수 있는 중재를 시행한다면 환자의 구강건강을 전반적으로 개선하는데 효과가 있을 것이다. 그러나 지금까지 보고된 연구에 따르면 뇌졸중 환자의 구강관리방법이 모두 상이하고 충분한 정보를 제시하고 있지 못하고 있는 실정이므로, 뇌졸중 환자를 위한 전문가 개입과 평가 방법을 개발하는 것이 필요하다. 따라서 본 연구에서는 뇌졸중 입원환자와 관련한 특성 및 범위, 주요 개념들을 매핑하여 향후 임상적 방향을 제시할 수 있는 주제범위 문헌고찰[19]을 이용하여 뇌졸중 입원환자를 위한 전문가 구강위생관리와 구강기능관리의 중재방법과 평가방법을 파악함으로써 추후 전문가 구강관리프로그램 개발의 방향을 제공하고자 한다.
본 연구의 질문은 ‘뇌졸중 일반병동 입원환자의 구강관리 중재를 위한 국제 연구의 동향은 어떠한가?’와 ‘뇌졸중 일반병동 입원환자의 구강관리 중재연구에 어떠한 특성이 있는가?’로 선정하였다. 연구 질문에서 인구집단(Population)은 뇌졸중 환자(성인과 노인), 개념(Concept)은 구강위생관리와 구강기능관리, 평가, 중재, 맥락(Context)은 일반병동(병원)으로 선정하였다.
연구검색은 2023년 7월 6일부터 2023년 9월 22일까지 이루어졌으며, 검색 시기는 2013년 1월 1일부터 2023년 7월 31일까지 최근 10년간 게재된 국제학술지 논문을 대상으로 하였다. 2명의 독립된 연구자가 연구고찰과 회의를 통해 검색 전략을 수립하여 연구질문에 따라 검색어를 설정하였다, 연구검색에 사용한 온라인 데이터베이스는 Cochrane, Embase, Medline, PubMed, ProQuest이며, 검색어는 데이터베이스의 부울 연산자(AND / OR)와 MeSH (Medical Subject Heading)용어를 사용하였고, 도출된 검색어와 검색식은 각 데이터베이스에 맞게 적용하였다<Appendix 1>.
stroke, oral hygiene, oral health, dental care
stroke, dysphagia, rehabilitation, oral function, exercise
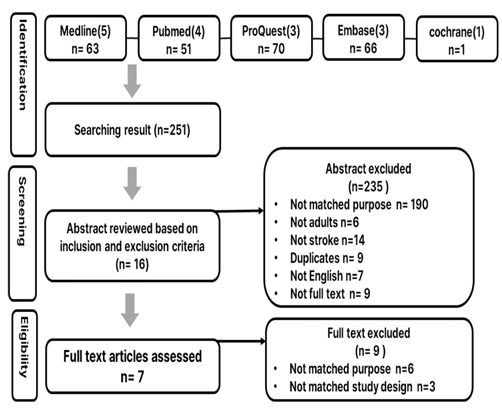
Fig. 1. Flowchart of the literature search and research process for OHM
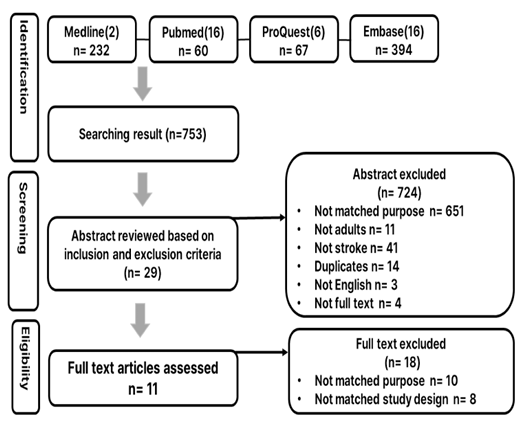
Fig. 2. Flowchart of the literature search and research process for OFM
2013년 1월 1일부터 2023년까지 7월 31일까지 국제학술지에서 2인의 연구자가 독립적으로 초록을 검토하였을 때 서로 간의 이견이 없었다. 먼저 제목과 초록을 검토하고 중복된 논문은 배제하였고, 포함기준은 뇌졸중 입원환자(성인과 노인), 임상시험, 중재연구, 국제학술지, 영어로 출판된 연구로 하였다. 배제기준은 중복되는 논문, 학위논문, 학술대회 발표 자료, 단행본, 원문의 전문이 없는 연구, 중재가 포함되지 않은 연구, 구강과 관련성 없거나 특정 질환에 편중된 연구, 급성 뇌졸중, 치매, 파킨슨병, 특정 질환 대상, 19세 미만 대상이었다.
2명의 연구자가 데이터베이스에서 검색한 결과, 구강위생관리는 총 251편 중 Medline 63편 PubMed 51편, ProQuest 70편, Embase 66편, Cochrane 1편의 논문이 확인되었고, 구강기능관리는 총 753편 중 Medline 232편, PubMed 60편, ProQuest 67편, Embase 394편이 확인되었다. 선별 과정에서 구강위생관리는 목적이 맞지 않는 연구 190편, 만성 뇌졸중 환자가 아닌 연구 14편, 선별기준에 포함되지 않는 연구(19세 미만인 자, 영어가 아닌 언어, 전문(full-text)이 없는 연구) 22편, 중복된 연구 9편을 제외하였고, 구강기능관리는 목적이 맞지 않는 연구 651편, 뇌졸중 환자가 아닌 연구 41편, 선별기준에 포함되지 않는 연구(위와 동일함) 18편, 중복된 연구 14편을 제외하였다. 최종 선정과정에서 구강위생관리는 16편, 구강기능관리는 29편의 전문을 확인하였으며, 연구목적과 관련성이 있는지 2차로 전문을 확인 후, 목적과 결과에 맞지 않는 연구를 각각 9편과 18편을 제외하여 최종 선정된 연구는 구강위생관리 7편과 구강기능관리 11편이었다<Fig.1,2, Appendix 2>.
최종 선정된 18편의 연구에서 자료를 추출하기 위해 Microsoft excel 프로그램을 사용하여 내용을 정리하였다<Table 1>. 첫째, 선정된 연구의 출판 관련 특성을 분석하였으며, 구강위생관리와 구강기능관리의 사용된 일반적 특성 내용은 최종 선정된 연구, 저자, 년도, 연구가 수행된 국가, 연구 디자인, 연구대상자, 중재 제공자, 표본 크기로 구성하였다. 둘째, 선정된 연구방법에서 사용된 평가지표, 중재도구, 중재방법, 결과를 기준으로 구강위생관리 및 구강기능관리의 평가지표, 중재도구, 중재방법의 기준으로 분류하였다.
구강위생관리의 중재자는 간호사(N=3), 치과조무사(N=2), 간병인(N=2)이었으며. 구강기능관리의 중재자는 언어병리학자(N=4), 작업치료사(N=4), 언어치료사(N=1), 치과위생사(N=1), 기타(N=1) 순이었다<Table 1>. 또한, 논문의 주저자를 기준으로 연구를 발표한 학문 분야를 분류하였을 때, 구강위생관리는 치의학(N=4, 57.1%)에서 가장 많이 수행되었고, 구강기능관리는 재활의학(N=5, 45.4%)이 가장 많았다<Fig. 3>.
Table 1. General characteristics of oral care study on stroke inpatients
| No. | 1st author (year) country | Participants (N) | Oral care provider | Study design, Intervention period, Purpose | ||
|---|---|---|---|---|---|---|
| Oral hygiene (N=7) | A1 | Purpose | Patients with stroke (N=81) | Nursing care aides | ⦁Single-blind, RCT ⦁3 weeks ⦁To evaluate the effectiveness of oral health interventions | |
| A2 | Lam OL (2013) Hongkong | Stroke patient undergoing rehabilitation (N=102) | Nursing care aides | ⦁Single-blind, RCT ⦁3 weeks ⦁To evaluate the effectiveness of oral health promotion interventions | ||
| A3 | Chipps E (2014) USA | Patients with stroke (N=51) | Nurse | ⦁RCT ⦁10 days ⦁To evaluate the effectiveness of oral care protocols in stroke patients | ||
| A4 | Kuo YW (2016) Taiwan | Patients with stroke (N=94) | Nurse | ⦁Single-blind, RCT ⦁2 months ⦁To evaluate the effectiveness of oral care training programs for stroke patients | ||
| A5 | Ab Malik N (2017) Malaysia | Patients with stroke (N=54) | Dental Assistant | ⦁RCT ⦁6 months ⦁To evaluate and compare the effectiveness of oral health promotion interventions | ||
| A6 | Ab Malik N (2018) Malaysia | Patients with stroke (N=76) | Dental assistant | ⦁RCT ⦁6 months ⦁To evaluate opportunistic pathogens before and after oral health care intervention | ||
| A7 | Chen HJ (2019) Taiwan | Patients with stroke and dysphagia (N=66) | Nurse | ⦁RCT ⦁12 weeks ⦁To evaluate the effectiveness of oral health programs before swallowing treatment. | ||
| Oral function (N=11) | A8 | Steele CM (2016) Canada | Patients with stroke (N=26) | Speech-Language Pathologists (S-LPs) | ⦁RCT ⦁3 months ⦁To compare the results of two tongue resistance training protocols | |
| A9 | Koyama Y (2017) Japan | Stroke patients with dysphagia (N=16) | Speech-Language Pathologists (S-LPs) | ⦁RCT ⦁6 weeks ⦁To validate the validity and effectiveness of jaw opening exercises | ||
| A10 | Choi JB (2017) Korea | Stroke patients with dysphagia (N=32) | Occupational therapist | ⦁RCT ⦁4 weeks ⦁To examine the effects of Shaker exercise | ||
| A11 | Hwang NK (2019) Korea | Stroke patients with dysphagia (N=21) | Occupational therapist | ⦁RCT ⦁4 weeks ⦁To examine the effectiveness of tongue stretching exercises | ||
| A12 | Liaw, MY (2020) Taiwan | Patients with stroke (N=21) | Technical | ⦁Prospective, RCT ⦁6 weeks ⦁Efficacy investigation (RMT, swallowing function, pulmonary function, functional performance) | ||
| A13 | Choi JB (2020) Korea | Stroke patients with dysphagia (N=21) | Occupational therapist | ⦁RCT ⦁6 weeks ⦁To investigate the thickness of the hyoid muscle and its effect on hyoid movement | ||
| A14 | Park JS (2020) Korea | Stroke patients with dysphagia (N=40) | Occupational therapist | ⦁RCT ⦁4 weeks ⦁To examine the effectiveness of JOE | ||
| A15 | Hägglund P (2020) Sweden | Stroke patients with dysphagia (N=44) | Nurse, Speech-Language Pathologists (S-LPs) | ⦁RCT ⦁5 weeks ⦁To verify that it improves swallowing capabilities | ||
| A16 | Shiraisi A (2021) Japan | Patients with stroke (N=300) | Dental hygienist | ⦁Retrospective cohort study ⦁111 days ⦁To examine the link between improved oral health and functional outcomes | ||
| A17 | Krekeler BN (2023) USA | Stroke patients with dysphagia (N=19) | Speech- Language Pathologists (S-LPs) | ⦁RCT ⦁12 weeks ⦁To examine the efficacy of tongue resistance training | ||
| A18 | Farpour S (2023) Iran | Patients after stroke (N=44) | Speech therapist | ⦁RCT ⦁4 weeks ⦁To investigate the effectiveness of SMG stimulation |
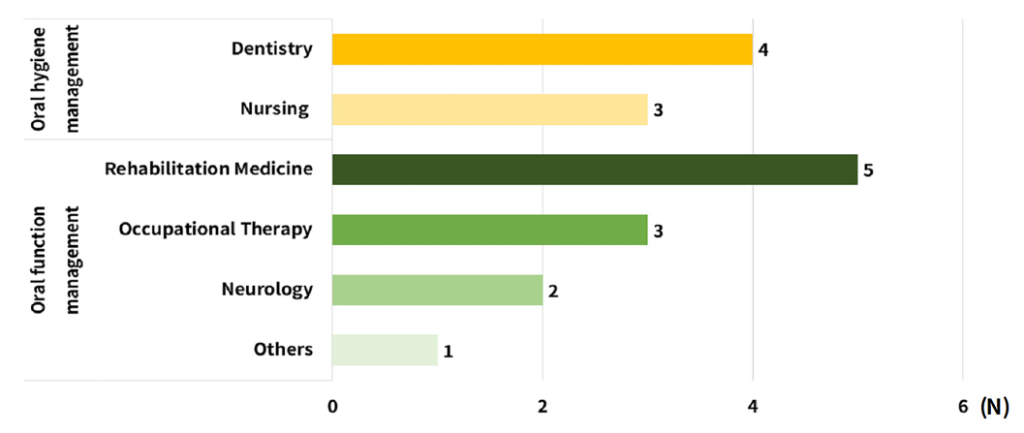
Fig. 3. Major academic fields conducting clinical research on oral hygiene management and oral function management for stroke inpatients
뇌졸중 환자의 구강위생관리에 사용한 평가지표는 치태지수(N=4), 치은출혈지수(N=2)이었고, 중재에 사용한 도구는 전동칫솔(N=5), 구강양치액(N=5), 수동칫솔(N=3)순으로 사용 빈도가 높았으며, 중재방법은 전문가가 수행하는 구강관리가 4편, 구강위생교육 실시 4편, 팜플렛만 제공한 경우가 4편이었다<Table 2>.
Table 2. Assessment, intervention tools, and methods of oral hygiene management research for stroke inpatients
(N=7)
| Division | N | Study | |
|---|---|---|---|
| Assessment | PI | 4 | ⦁Silness and Loe: A1, A5 ⦁PI: A2, A4 (index were not presented) |
| GBI | 2 | A1, A2 | |
| DMFT | 1 | A2 | |
| THROAT | 1 | ⦁R-THROAT: A3 | |
| TC | 1 | ⦁WTCI: A4 | |
| OHAT | 1 | A7 | |
| Intervention tool | Electric toothbrush | 5 | A1, A2, A3, A5, A6 |
| Mouth rinse | 5 | ⦁CHX 0.2%, 10 mL: A1, A2 ⦁Listerine 10-15 mL: A3 ⦁1% CHX oral gel: A5, A6 | |
| Toothbrush | 3 | A1, A2, A4 | |
| Toothpaste | 2 | A1, A3 | |
| Tongue cleaner | 2 | A3, A4 | |
| Dental floss | 2 | A3, A7 | |
| Interdental brush | 1 | A7 | |
| Lip balm | 1 | A3 | |
| Intervention method | POHC | 4 | A1, A4, A6, A7 |
| pamphlet | 4 | A4, A5, A6, A7 | |
| OHI | 4 | A1, A2, A4, A5 |
PI: Plaque Index; GBI: Gingival Bleeding Index; DMFT: The Decayed, Missing and Filled Teeth; THROAT: The Holistic and Reliable Oral Assessment Tool; R-THROAT: Revised-The Holistic and Reliable Oral Assessment Tool; TC: Tongue Coating; WTCI: Winkel Tongue Coating Index; OHAT: Oral Health Assessment Tool; POHC: Professional Oral Hygiene Care; OHI: Oral Hygiene Instruction
뇌졸중 환자의 구강기능을 향상시키기 위해 사용한 평가지표는 기능적 경구섭취척도(FOIS, N=6), 비디오투시연하검사(VFSS, N=6), 침습흡인 척도(PAS, N=5)가 많이 사용되고, 중재는 전통적인 운동 방법과 장비를 이용한 훈련으로 분류할 수 있었으며 연구마다 서로 다른 중재법을 적용하였는데, 그 중에 빈도가 가장 높은 중재법은 턱벌림운동(JOE, N=3)과 혀압력(TP, N=3)이었다<Table 3>.
Table 3. Assessment and in tervention methods of oral function management research for stroke inpatients (N=11)
| Division | N | Study | |
|---|---|---|---|
| Assessment | FOIS | 6 | A9, A10, A12, A14, A17, A18 |
| VFSS | 6 | A8, A9, A11, A14, A15 A16 | |
| PAS | 5 | A8, A10, A14, A15, A17 | |
| MASA | 3 | A8, A17, A18 | |
| NIHSS | 3 | A1, A17, A18 | |
| SWAL-QOL | 2 | A8, A17 | |
| MIP | 2 | A1, A8 | |
| TWST | 1 | A16 | |
| BI | 1 | A12 | |
| BRPES | 1 | A13 | |
| NG tube remove rate | 1 | A14 | |
| LF | 1 | A15 | |
| TWST | 1 | A15 | |
| CCI | 1 | A16 | |
| mRS | 1 | A16 | |
| ROAG | 1 | A16 | |
| FIM | 1 | A16 | |
| MNA-SF | 1 | A16 | |
| SMI | 1 | A16 | |
| MMSE | 1 | A17 | |
| NRRS | 1 | A18 | |
| Intervention methods | JOE | 3 | ⦁MJOE: A9 ⦁JOE: A13 ⦁RJOE: A14 |
| TP | 3 | ⦁TPPT, TPSAT: A8 ⦁Resistance tongue exercise pressure (using the device): A17 ⦁TSE: A11 | |
| Orofacial sensory stimulation | 2 | ⦁Oral device (neuromuscular), electric toothbrush (use of vibration): A15 ⦁Ice massage, jelly: A16 | |
| SE | 1 | A10 | |
| Dolfin breathing trainer | 1 | A12 | |
| HLE | 1 | A13 | |
| tDCS | 1 | A18 |
FOIS: Functional Oral Intake Scale; VFSS: Video Fluoroscopic evaluation Swallow Study; PAS: Penetration Aspiration Scale; MASA: Mann Assessment of Swallowing Ability; NIHSS: National Institutes of Health Stroke Severity; SWAL-QOL: Swallowing Quality of Life; MIP: Maximum Isometric Pressure; TWST: Timed Water-Swallow Test; BI: Barthel Index; BRPES: Borg Rating of Perceived Exertion Scale; NG tube remove rate: Nasogastric tube remove rate; LF: Lip-Force test; CCI: Charlson Comorbidity Index; mRS: modified Rankin Scale; ROAG: Revised Oral Assessment Guide; FIM: Functional Independence Measure; MNASF: Mini Nutritional Assessment Short-Form; SMI: Skeletal Muscle mass Index; MMSE: Mini-Mental State Examination; NRRS: Normalized Residue Rating Scale; JOE: Jaw Opening Exercise; TP: Tongue-Pressure; SE: Shaker Exercise; HLE: Healthy Life Expectancy; tDCS: transcranial Direct Current Stimulation; MJOE: Modified Jaw Opening Exercise; RJOE: Resistive Jaw Opening Exercise; TPPT: Tongue-Pressure Profile Training; TPSAT: Tongue-Pressure Strength and Accuracy Training
본 연구는 뇌졸중 환자의 구강위생관리와 구강기능관리의 평가와 중재방법에 관한 논문 총 18편을 선정하여 주제범위 문헌고찰 방법으로 분석함으로써 뇌졸중 환자를 위한 치과위생사의 전문가 구강관리프로그램의 개발 방향을 수립하기 위해 실시하였다.
뇌졸중 환자의 구강위생관리에 관한 중재연구의 동향을 분석한 결과, 2013년부터 2017년까지 출판된 논문은 5편이었고, 2018년부터 2021년까지 출판된 논문은 2편이었다. 뇌졸중 환자를 연구 대상으로 하여 구강위생관리 연구를 수행한 연구자의 소속 국가는 총 4개국(대만, 말레이시아, 미국, 홍콩)에 국한되었고, 구강관리를 시행한 중재자는 간병인, 간호사, 치과 보조원이었다. 구강위생관리 중재연구를 수행한 국가 중 말레이시아는 치과보조원이 포함되어 있었는데, 말레이시아에서는 치과보조원 취득과정이 학교에서 2년 이론교육과 1년 실습을 거쳐 자격시험을 취득하여 전문적인 치과진료 보조업무를 담당할 수 있는 직업으로 명시하고 있다. 명칭은 다르지만, 실질적인 업무와 취득과정은 우리나라의 치과위생사와 유사한 형태로 판단된다. 치과위생사가 중재자로 현저하게 적은 이유는 치과위생사의 국가별 업무 범위의 차이뿐만 아니라 뇌졸중 환자들이 주로 입원 병동에 있는 것에 의해 접근성이 낮았기 때문으로 유추된다.
구강기능관리 연구는 총 7개국(미국, 이란, 일본, 스웨덴, 캐나다, 대만, 한국)에서 수행되었고, 연구 참여자는 뇌졸중 환자, 삼킴 장애가 있는 뇌졸중 환자, 뇌졸중 후 환자로 규정되어 있었다. 구강기능을 개선하기 위한 중재자로서 작업치료사, 언어병리학자, 언어치료사, 간호사, 치과위생사 순으로 나타나 여러 직종에 의해 연구가 수행되고 있었다. 주로 작업치료사와 언어병리학자 등과 같이 종합병원급의 의료시설 근무자에 의해 많이 수행된 이유로는 뇌졸중 입원환자를 접할 수 있는 환경적 이점이 있기 때문이라고 생각할 수 있다. 그러나 향후 전문적 지식을 갖춘 학문 분야 간의 융합을 통해 입원환자의 특성에 맞는 중재도구 및 평가지표 개발이 필요할 것이다.
뇌졸중 환자를 위한 전문가 구강관리 프로그램을 개발하기 위해 선행연구에서 사용한 평가지표를 분류하였을 때, 구강위생관리 연구에서는 치태지수와 치은출혈지수를 가장 많이 사용하고 있었다. 그리고 구강위생관리의 중재도구는 전동칫솔과 구강양치액이 각각 5개 연구에서 사용되어 가장 빈도가 높았다. 뇌졸중 환자에게 클로르헥시딘을 사용하여 구강관리를 시행한 연구[21]에서 클로르헥시딘을 사용한 그룹이 대조군에 비해 폐렴의 발생을 유의하게 감소시켰고, 전동칫솔과 0.2% 클로르헥시딘, 그리고 치약 및 구강위생관리 지침을 제공하는 고급 구강위생 관리프로그램의 효과를 평가한 연구[22]에서는 고급 구강위생관리 프로그램을 받은 경우 기존 구강위생 관리프로그램에 비해 환자의 구강건강이 개선되고, 치태 및 치은 출혈이 현저하게 줄어들었다고 보고하였다. 즉, 전문적인 중재방법을 통해 환자의 구강위생 상태를 향상시킬 수 있다는 것을 의미한다. 구강기능관리 연구에서 활용한 평가지표는 FOIS, PAS, VFSS 순으로 나타났다. 연구 중재방법은 턱벌림운동(JOE), 혀압력(TP)이 가장 많이 사용되었고, 중재방법는 턱벌림운동과 혀 압력훈련장비, 구강 및 안면 자극도구 이었다. 구강은 저작과 연하에 관련된 근육과 구강 건조 등 복합적으로 작용하여, 연령이 증가하면서 신체 허약할수록 구강 기능이 감소하게 된다[23]. 따라서 노인이나 신체기능이 감소한 입원환자에게 손상된 구강기능을 향상시키기 위해 구강재활운동을 적용하는 것이 필요하다[24]. 구강운동을 실시했을 때 건강한 노인은 구강기능 수준이 향상되었고, 구강 기능이 저하된 노인은 구강건강의 회복과 유지가 되었으며, 전반적으로 연구 참여 노인의 구강기능과 구강건강 관련 삶의 질이 향상되었다[25]. 또한, 3개월 동안 구강기능향상운동 프로그램과 치과위생사의 관리를 제공했을 때 재가 노인의 타액분비량, 구강건강과 삶의 질, 구강기능을 향상에 효과가 있는 것으로 나타났다[26]. 그리고 치과위생사가 전문요양시설 노인들의 구강기능관리를 시행하여 구강기능점수(구강습윤도, 구륜근력, 교합력, 연하력)가 모두 향상되었다는 연구 결과도 보고된 바 있다[27]. 2006년부터 일본에서는 개호예방사업 중 하나로 구강기능향상이 되도록 사업을 추진하여 효과를 입증하였고, 참여한 전문인력은 간호사, 언어병리사, 치과위생사 등 포함되었다[28]. 앞서 언급한 선행연구의 사례들을 보면 전문적 구강기능관리를 통해 구강기능이 개선될 수 있었다. 따라서 최근 입원환자와 고령자에 대한 관심이 높아지고 있는 우리나라에서도 전문적인 구강관리 프로그램 개발을 위한 지속적인 관심과 연구가 필요할 것이다.
본 연구는 주제범위 문헌고찰의 연구방법을 통해 뇌졸중 환자의 구강관리 중재연구의 일반적 특성과 사용도구, 방법을 분류함으로써 현재 뇌졸중 환자의 구강관리 중재연구에 동향을 파악하고 향후 치과위생사에 의한 전문 구강관리프로그램 개발을 위한 연구의 방향성을 제시하고자 하였다. 그러나 본 연구에서는 다음과 같은 제한점을 가지고 있다. 첫째, 뇌졸중 환자를 위한 평가와 중재방법은 무작위 대조군 연구만을 대상으로 하였으므로 총 18편(구강위생관리 7편/ 구강기능관리 11편)으로 연구의 수가 적어 결과를 일반화하기에 어려움이 있었다. 연구검색 단계에서 무작위 대조군 연구를 선정하는 과정에서 많은 논문이 배제되었다. 그러나 논문의 기초정보를 활용하여 추후 연구 방향을 모색하기 위한 목적으로 수행하였기 때문에 연구의 목적에 따라 무작위 대조군 연구로만 한정하였다. 둘째, 본 연구에서는 국제학술지에 게재된 논문으로 제한하였으므로 국내 학술논문, 학위논문, 정책 보고서, 학술대회 자료, 전문이 없는 연구 등 모두 제외하였고, 원문제공서비스의 공개가 제한적인 경우가 많아 연구에 포함시키는데 어려움이 있었다. 그러나 본 연구는 뇌졸중 입원환자를 무작위로 배정하여 전문가 구강위생관리 또는 전문가 구강기능관리를 시행한 국외 연구 현황들을 검토하여 연구 방향을 구체적으로 알 수 있다는 점에 의의가 있다. 본 연구의 결과를 토대로 향후 연구에서는 치위생학 분야 및 치과위생사들은 중재방법 및 평가지표 개발과 임상에서 활용하기 위해 뇌졸중 환자의 삼킴장애가 있는 연구대상자에 대한 이해 및 관심이 필요할 것으로 생각된다.
본 연구는 2013년부터 2023년까지 주제범위 문헌고찰을 이용하여 뇌졸중 환자에게 적용할 수 있는 구강위생관리와 구강기능관리의 중재방법 및 평가지표를 확인함으로써 전문구강관리의 동향을 알아보았다.
1. 뇌졸중 환자 및 삼킴 장애가 있는 뇌졸중 환자를 대상으로 한 연구는 총 18편을 선정하였으며, 구강위생관리에 관한 연구는 7편이었고, 구강기능관리에 관한 연구는 11편이었다.
2. 구강위생관리 평가지표는 치태지수와 치은출혈지수를 가장 많이 사용하였고, 중재도구와 방법은 전동칫솔, 구강양치액, 전문가 구강관리제공이 있었다.
3. 구강기능관리 평가는 FOIS, VFSS, PAS를 많이 사용하였고, 중재도구와 방법은 턱벌림운동과 혀 압력훈련장비, 구강 및 안면 자극도구를 활용하였다.
치위생학과와 치의학 분야에서는 뇌졸중 환자의 전문 구강관리에 대한 연구가 부족하여 뇌졸중 환자를 위한 구강관리 방법의 기준을 설정하는 데 한계가 있으며, 이를 명확히 하기 위해서는 평가지표의 확대가 필요하다. 구강위생관리와 구강기능관리는 뇌졸중 환자에게 중요한 요소이기 때문에 추후 적절한 중재방법과 평가지표를 개발하여 적용하기 위한 준비가 필요할 것이다.
Conceptualization: SM Kim, EB Cho, SY Han; Data collection: SM Kim, EB Cho; Formal analysis: SM Kim, SY Han; Writingoriginal draft: SM Kim, SY Han; Writing-review&editing: SM Kim, EB Cho, SY Han
The authors declared no conflicts of interest.
This research was supported by ‘Regional Innovation Strategy (RIS)’ through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) (2022RIS-005).
None.
There are no relevant issues, but the data can be obtained from the corresponding author.
None.
1. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke 2005;36(12):2756-63. https://doi.org/10.1161/01.STR.0000190056.76543.eb
[DOI][PubMed]
2. Hong KS, Kang DW, Koo JS, Yu KH, Han MK, Cho YJ, et al. Impact of neurological and medical complications on 3-month outcomes inacute ischaemic stroke. European Journal of Neurology 2008;15(12):1324-31. https://doi.org/10.1111/j.1468-1331.2008.02310.x
[DOI][PubMed]
3. Pow EH, Leung KC, Wong MC, Li LS, McMillan AS. A longitudinal study of the oral health condition of elderly stroke survivors on hospital discharge into the community. International Dental Journal 2005;55(5):319–24. https://doi.org/10.1111/j.1875-595X.2005.tb00330.x
[DOI][PubMed]
4. Kim EK, Kim MS, Lee HK. A study on the oral health and oral health related quality of life of stroke patients in a rehabilitation ward: a pilot study. J Dent Hyg Sci 2016;16(2):127-33. https://doi.org/10.17135/jdhs.2016.16.2.127
[DOI]
5. Sørensen, RT, Rasmussen RS, Overgaard K, Lerche A, Johansen AM, Lindhardt T. Dysphagia screening and intensified oral hygiene reduce pneumonia after stroke. J NeurosciNurs 2013;45(3):139-46. https://doi.org/10.1097/JNN.0b013e31828a412c
[DOI][PubMed]
6. Kim EK, Park EY, Sa Gong JW, Jang, SH, Choi YH, Lee HK. Lasting effect of an oral hygiene care program for patients with stroke during in-hospital rehabilitation: a randomized single-center clinical trial. Disability and Rehabilitation 2017;39(22):2324-9. https://doi.org/10.1080/09638288.2016.1226970
[DOI][PubMed]
7. Talbot A, Brady M, Furlanetto DL, Frenkel H, Williams BO. Oral care and stroke units. Gerodontology 2005;22(2):77-83. https://doi.org/10.1111/ j.1741-2358.2005.00049.x
[DOI][PubMed]
8. Horne M, McCracken G, Walls A, Tyrrell PJ, Smith CJ. Organisation, practice and experiences of mouth hygiene in stroke unit care: a mixedmethods study. J Clin Nurs 2015;24(5-6):728–38. https://doi.org/10.1111/jocn.12665
[DOI][PubMed]
9. Daramola T. The Ohio State University[Doctoral dissertation]. Columbus: The Ohio State University, 2010.
10. Lee YJ, Noh HJ, Han SY, Jeon HS, Chung WG, Mun SJ. Oral health care provided by nurses for hospitalized patients in Korea. Int J Dent Hyg 2019;17(4):336-42. https://doi.org/10.1111/idh.12417
[DOI][PubMed]
11. Lalla E, Papapanou PN. Diabetes mellitus and periodontitis: a tale of two common interrelated diseases. Nat Rev Endocrinol 2011;7(12):73848. https://doi.org/10.1038/nrendo.2011.106
[DOI][PubMed]
12. Jang JH, Cho JW, Kim YJ, Ki JY, Jo KS, Kim JR, et al. Preliminary study for the development of a visiting oral health care intervention program for the elderly based on community healthcare. J Korean Acad Oral Health 2020;44(3):166-72. https://doi.org/10.11149/jkaoh.2020.44.3.166
[DOI]
13. Choi MI, Han SY, Jeon HS, Choi ES, Won SE, Lee YJ, et al. The influence of professional oral hygiene care on reducing ventilator-associated pneumonia in trauma intensive care unit patients. Br Dent J 2022;232(4):253-9. https://doi.org/10.1038/s41415-022-3986-3
[DOI][PubMed]
14. Fan D, Lee YH, Lee HK. The effect of oral hygiene care program in stroke patients. J Korean Soc Dent Hyg 2014;14(3):363-70. https://doi.org/10.13065/jksdh.2014.14.03.363
[DOI]
15. Suzuki R, Nagano A, Wakabayashi H, Maeda K, Nishioka S, Takahash M, et al. Assignment of dental hygienists improves outcomes in Japanese rehabilitation wards: a retrospective cohort study. J Nutr Health Aging 2020;24(1):28-36. https://doi.org/10.1007/s12603-019-1284-9
[DOI][PubMed]
16. Bang HL, Park YH. The effect of an exercise-based swallowing training program for nursing home residents with stroke. J Muscle Jt Health 2014;21(2):85-96. https://doi.org/10.5953/JMJH.2014.21.2.85
[DOI]
17. Arnold M, Liesirova K, Broeg-Morvay A, Meisterernst J, Schlager M, Mono ML, et al. Dysphagia in acute stroke: incidence, burden and impact on clinical outcome. PLoS ONE 2016;11(2):e0148424. https://doi.org/10.1371/journal.pone.0148424
[DOI][PubMed][PMC]
18. Kim HS, Lim KC. Effects of swallowing training program for nursing home residents with stroke. J Muscle Jt Health 2023;30(3):230-41. https://doi.org/10.5953/JMJH.2023.30.3.230
[DOI]
19. Levac D, Colquhoun H, O’brien KK. Scoping studies: advancing the methodology. Implement Sci 2010;20(5):1-9. https://doi.org/10.1186/1748-5908-5-69
[DOI][PubMed][PMC]
20. Arksey H, O’Malley L. Scoping studies: toward a methodological framework. Int J Soc Res Methodol 2005;8(1):19-32. https://doi.org/10.1080/1364557032000119616
[DOI]
21. Labeit B, Michou E, Trapl-Grundschober M, Suntrup-Krueger S, Muhle P, Bath PM, et al. Dysphagia after stroke: research advances in treatment interventions. The Lancet Neurology 2024;23(4):418-28. https://doi.org/10.1016/S1474-4422(24)00053-X
[DOI][PubMed]
22. Dai R, Lam OL, Lo EC, Li LS, McGrath C. A randomized clinical trial of oral hygiene care programmes during stroke rehabilitation. J Dent 2017;(61):48-54. https://doi.org/10.1016/j.jdent.2017.04.001
[DOI][PubMed]
23. Lee GR, Kim DR, Lim HN, Kang KH. The effects of the oral care program for improving swallowing function of the elderly using welfare centers on depression, self efficacy, subjective oral health status and swallowing related quality of life. Res Community Public Health Nurs 2020;31(2):166-78. https://doi.org/10.12799/jkachn.2020.31.2.166
[DOI]
24. McKenna G, Allen PF, Hayes M, DaMata C, Moore C, Cronin M. Impact of oral rehabilitation on the quality of life of partially dentate elders in a randomized controlled clinical trial: 2year follow-up. PLoS ONE 2018;13(10):e0203349. https://doi.org/10.1371/journal.pone.0203349
[DOI][PubMed][PMC]
25. Cho EP. Impact of oral function improving exercise on the oral function and quality of life in the elderly[Doctoral dissertation]. Daejeon: Chungnam National University, 2009.
26. Yang SO, Jeong GH, Kim SJ, Kim KW, Lee SH, Saung SY, et al. The effects of oral function improving exercise on the UWS, oral function and OHIP in elderly. J Korean Pubilc Health Nurs 2012;26(3):478-90. https://doi.org/10.5932/JKPHN.2012.26.3.478
[DOI]
27. Kim YS, Shin KH, Park JR, Chung SH, Choi HS. The effect of oral function improvement with oral exercise program by elderly people. J Korean Soc Dent Hyg 2016;16(4):559-66. https://doi.org/10.13065/jksdh.2016.16.04.559
[DOI]
28. Sakayori T, Maki Y, Hirata S, Okada M, Ishii T. Evaluation of a Japanese “prevention of long-term care” project for the improvement in oral function in the high-risk elderly. Geriatr Gerontol Int 2013;13(2):451-7. https://doi.org/10.1111/j.1447-0594.2012.00930.x
[DOI][PubMed]
Appendix 1. Search expression and results
table
*Duplicates were removed and documents that were not relevant to the research topic, such as publication year, were organized accordingly.
table
Appendix 2. Literature review
table