
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Susanne Sunell![]() , Zul Kanji
, Zul Kanji![]()
Oral Biological & Medical Sciences, Faculty of Dentistry, The University of British Columbia
Correspondence to Susanne Sunell, Oral Biological & Medical Sciences, Faculty of Dentistry, The University of British Columbia, 2199 Wesbrook Mall, Vancouver, BC V6T 1Z3, Canada. Tel: 604-822-5747, E-mail: susunell@dentistry.ubc.ca
Volume 25, Number 6, Pages 473-85, December 2025.
J Korean Soc Dent Hyg 2025;25(6):473-85. https://doi.org/10.13065/jksdh.2025.25.6.2
Received on November 17, 2025, Revised on December 16, 2025, Accepted on December 17, 2025, Published on December 30, 2025.
Copyright © 2025 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: The curriculum redesign process within the University of British Columbia’s (UBC) Dental Hygiene Degree Program (DHDP) involved the creation of new curriculum in social entrepreneurship, advocacy, and interprofessional education. Thus the research question was: where can curriculum spaces be found for the new renewal themes? Methods: The DHDP course and section coordinators (n=16) were invited to a three-round Delphi study to explore curriculum spaces. Round 1 asked participants to identify curriculum spaces. Round 2 asked participants to rate their agreement with the round 1 items. Round 3 asked participants to rank items for implementation. Results: The response rate was 81% in round 1, 56% in round 2, and 69% in round 3. Consensus was reached to create spaces within (a) biomedical sciences, (b) statistics, oral epidemiology, and literature reviews, and (c) theory and practice. Twenty-six hours were found for social entrepreneurship and 24 hours for advocacy curriculum. Conclusions: Curriculum spaces were found but the redesign process can be challenging as faculty may experience a loss of their expertise. The findings of this study are specific to UBC’s program. However, the spaces found, and the lessons learned will likely resonate with faculty members across the health professions.
Baccalaureate degree, Curriculum design, Curriculum development, Delphi study, Dental hygiene education
The UBC Dental Hygiene Degree Program (DHDP) is a 4-Year Bachelor of Dental Science (Dental hygiene) degree (BDSc [DH]), was initially implemented in 1992 as an online degree completion program for diploma graduates to earn a degree specific to their profession. A further on-site 4-Year entry-to-practice academic pathway was then implemented in 2007.
In 2015 the Canadian Dental Hygienists Association (CDHA) published the first Canadian Competencies for Baccalaureate Dental Hygiene Programs (CCBDHP) [1]. They were integrated into the UBC DHDP in the 2016-2017 academic year. The integration of the national dental hygiene competencies was the impetus for an in-depth curriculum renewal exploration [2]. After conducting a gap analysis involving the newly established competencies, the faculty focused on gaining student input. The UBC dental hygiene faculty conducted a one-time survey of its graduates (2013 to 2016) [3] and a longitudinal study of the senior students in the entryto-practice pathway extending from 2017 to 2019 [4]. The program graduates and the 4th year graduating students were asked to rate their confidence level in the 13 competency domains of the CCBDHP [1]. In August 2019 a retreat was implemented including faculty, staff, alumni, and representatives of the provincial professional and regulatory organizations. During the 2019 retreat, consensus was reached on the need for an in-depth program renewal project with a focus on (1) inter-professional education, (2) advocacy & policy use, and (3) entrepreneurship & leadership. These themes were viewed as particularly important as a new registration class, Dental Hygiene Practitioner (DHP), was then established in March of 2020 allowing baccalaureate dental hygienists to establish practices as primary care providers.
The UBC dental hygiene renewal process is an example of backward design to guide curriculum revision of an existing program, also know as program ‘redesign’ [5]. This redesign started with the mapping process to the national baccalaureate competencies [1] and then focused on the three themes identified during the faculty retreat. To support the renewal process, a Curriculum Renewal Task Force (CRTF) was created in September 2021 with three focus groups tasked with the development of the associated competencies and learning outcomes [2].
Creating new curriculum is interesting and stimulating. However, finding curriculum spaces for enhanced knowledge and abilities is an ongoing challenge in post-secondary education as faculty members often have a vested interest in the subjects they facilitate [5] with administrators and politicians often being concerned about credential inflation [6-8]. The focus was to find instructional hours that could be repurposed within a course or shifted to another course to allow for the renewal learning outcomes to be integrated within the DHDP program. This was expressed as finding ‘curriculum spaces.’ This term allowed for a shift away from the concept of searching for ‘redundant’ curriculum and its possible negative context for faculty members. An important redesign initiative was already underway. It involved the modification of the first year Theory and Practice course from a three credit to a six-credit course to support an early introduction to community health curriculum including public health policy, advocacy, community health, and community engagement. It was organized as an intra-professional course involving both dental hygiene and dentistry students and it was uniquely positioned before the clinical curriculum commenced. While this was an initial opportunity to create spaces within the DHDP, other curriculum spaces needed to be found.
Five key articles for curriculum design were identified through a Delphi study; only one of these involved a program redesign process [9]. Three of the articles used Kern’s 6-step approach to support curriculum development [10]. The steps include an ‘implementation’ step focused on the procurement of resources including time [10-12]. However, no guidance was given as to how to find such time. Finding curriculum spaced was viewed as an essential but also challenging task. A UBC study by Best et al [13] used a Delphi approach to gain consensus on the ‘essential biomedical objectives’ within the UBC dentistry program. It illustrated the potential value of a Delphi approach, and the DHDP faculty moved forward to implement a 3 round Delphi from October 2021 to May 2022 to gain consensus on possible curriculum spaces available. This study provides a unique contribution to the discussion of curriculum redesign given its focus on finding curriculum spaces.
This Delphi study was implemented while the focus groups were meeting monthly to generate their respective curriculum [2]. The faculty members were concurrently immersed in creating new curriculum and identifying spaces for its accommodation. The parallel initiatives helped to emphasize the need to find curriculum spaces while maintaining the full scope of dental hygiene practice. This article reports the findings of the Delphi study.
This study aimed to identify possible curriculum spaces within the UBC DHDP to accommodate new renewal themes, using a 3-round Delphi approach. The following research question guided this Delphi study:
Where can we best find spaces for the curriculum themes while maintaining a balance supportive of the scope of practice of DHPs?
This question and its associated study protocols were approved by the University of British Columbia (UBC), Office of Research Ethics (#H21-02608) in the fall of 2021 and the Delphistar checklist was used to support methodological rigor (https://www.equatornetwork.org › reporting-guidelines).
A classic Delphi approach provided a structured group communication process to support decision-making [14-18] grounded in the expertise of the faculty members. It had the benefit of providing anonymity of responses and thus helped to avoid the ‘group think’ that often comes with face-to-face meetings. It allowed for the consideration of diverse perspectives and opportunities to question established ideas [18]. These benefits were seen as particularly relevant given the challenges of reducing established curriculum. The study involved a purposeful sampling approach. The dental hygiene course and section coordinators were invited to participate in the survey (n=16). These individuals had responsibility for course and/or course section design, implementation and evaluation. The DHDP includes large courses in Dental Hygiene Theory and Practice organized into sections with each section being delivered weekly over one term. These faculty members were in the best position to have a comprehensive overview of the curriculum. The other part-time dental hygiene faculty members were not included as their knowledge tended to be more narrowly focused.
An online Delphi survey instrument was organized into 3 rounds with the program courses organized into the following sections: Biomedical Sciences
Theory & Practice (including clinical and community practice)
Research & Epidemiology
Advocacy & Policy
Courses from Non-Dentistry Faculties
Round 1 asked respondent to identify spaces in the courses to allow for enhanced curriculum related to the renewal themes. They were also asked to identify possible pitfalls in the re-alignment of the curriculum. The data from round 1 were then used to generate a list of possible areas were curriculum spaces existed. Round 2 then asked respondents to rate the degree to which they agreed or disagreed with the suggestions arising from round 1. The round 2 data were then used as the basis for round 3 which asked respondents to rank the ideas within each of the sections and to add further comments regarding curriculum spaces.
Informed consent was initially gained in November of 2021 based on the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. The study was conducted online; respondents were informed that round 1 was anticipated to take about 2.5 hours with rounds 2 and 3 needing another hour each for a total of 4.5 hours of time. Respondents were provided 3.5 weeks to complete each round. Round 1 started in early November and round 3 finished in the middle of April 2022 with the Delphi report being available for faculty in May 2022. The Delphi report became a resource for an early June meeting including the course and section coordinators (i.e. the Delphi participants). <Fig. 1> for a schematic that highlights the context of the Delphi study within the overall program redesign.
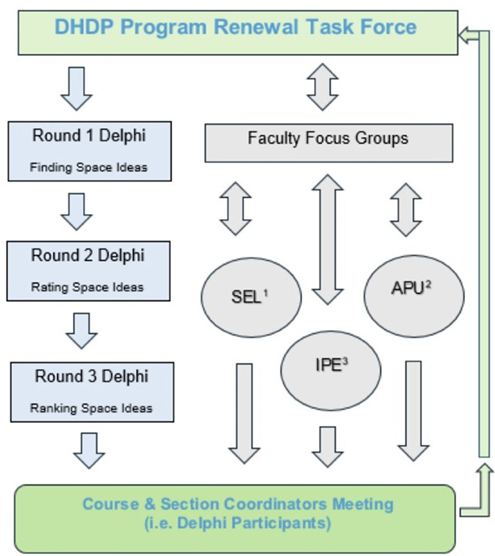
Fig. 1. Context of Delphi study within renewal process: December 2021 to June 2022.
1Social entrepreneurship and leadership, 2Advocacy and policy use, 3Inter-professional experiences.
Thematic analysis was used to explore the data from round 1 as well as the open-ended questions in round 2 and 3. It involved several stages of coding and recoding to explore similar and divergent views. The initial coding was conducted by the primary author and was then expanded to include the research assistant. A feedback loop was conducted at the end of each round to gain participants’ input. At the end of round 3 a face-to-face meeting was conducted with study participants to finalize the analysis <Fig. 1>. This final meeting in June 2022 focused on the validation of study results and involved the identification of the specific curriculum spaces available for renewal curriculum.
Descriptive statistical tests were conducted on the numeric data from round 2 and 3 using the IBM SPSS program (ver. 26.0; IBM Corp., Armonk, NY, USA) software. Inferential statistical tests were not employed as the study characteristics did not align with the assumptions that underpin inferential statistical tests. The research question of this study did not focus on exploring relationships between variables, either the direction or the strength of the relationship. It was directed to building consensus and such studies often include small number of respondents with unique/expert knowledge related to the research question.
Delphi studies normally include a predetermined consensus level; such levels often range from 51% to 80%, with 70% being a common standard [19]. Our study included a consensus level of 50% in round 3 to support the inclusion of diverse opportunities. While this level is reported in this article, in practice it was artificial given that the study participants had the opportunity to raise all possible options for curriculum spaces during the June 2022 meeting. The results section includes a combination of tables and the respondents’ views to provide insights as to how dental hygiene curriculum could be shaped to support redesign initiatives.
The response rate for the three Delphi rounds was 81% in round 1, 56% in round 2, and 69% in round 3. Each of the 3 Delphi rounds included several people teaching in each year of the 4 years degree program with higher numbers in years 2 to 4 inclusive. This is not surprising as Year 1 includes courses delivered through faculties other than Dentistry. Respondents’ highest educational credential included Master’s degrees or doctoral degrees. The great majority were DHPs but also included two dentists and another academic. Respondents’ teaching and/ or administrative experience ranged from 6 to over 26 years. They were viewed as having the content expertise to provide meaningful input.
Table 1. Delphi respondents’ demographics
| Respondents’ demographics | Rounds of delphi study | ||
|---|---|---|---|
| Round 1 | Round 2 | Round 3 | |
| Number of respondents/round (n=16) | 81% n=13 |
56% n=9 |
69% n=11 |
| Year of program in which teaching (yr) | |||
| 1 | 4 | 2 | 5 |
| 2 | 10 | 6 | 8 |
| 3 | 8 | 7 | 9 |
| 4 | 10 | 7 | 9 |
| DMD | 2 | 1 | 1 |
| Highest educational credential | |||
| Master’s degree | 8 | 4 | 6 |
| Academic doctorate | 4 | 3 | 5 |
| Professional doctorate | 1 | 1 | |
| Oral health professional designations | |||
| Dental hygiene practitioner | 10 | 6 | 8 |
| DMD/DDS | 2 | 1 | 1 |
| Not applicable | 1 | 2 | 2 |
| Years of teaching and/or administrative experience | |||
| Between 6 and 10 years | 2 | 2 | 1 |
| Between 11 and 15 years | 5 | 2 | 3 |
| Between 16 and 20 years | 2 | 1 | 3 |
| Between 21 and 25 years | 3 | 1 | 1 |
| Over 26 years | 1 | 2 | 3 |
Round 1 recommendation became the basis for the round 2 survey that asked respondents to rate their agreement with each of the round 1 items. The data from round 2 <Table 2,3> present the agreement rating data and round 3 provides ranking data <Table 4,5>. The Delphi included program specific course names which have been changed to a generic content name to support greater understanding by diverse readers.
Table 2. Summary of round 2 agreement ratings from the perspective of the course content in the Biomedical Sciences and Theory & Practice courses
| DHDP proposed renewal spaces | Agreement ratings in % with ‘n’ in brackets |
||
|---|---|---|---|
| Agree | Strongly agree | Total | |
| DHDP Biomedical Sciences (n=10) | |||
| A1. Explore overlap in Oral Health Sciences 1 (OHS 1) and Oral Health Sciences 2 (OHS 2) | 60(6) | 20(2) | 80 |
| A2. Explore overlap in Dental Anatomy and Head & Neck Anatomy | 30(3) | 40(4) | 70 |
| A3. Reassess the knowledge in embryology sessions in Head & Neck Anatomy | 10(1) | 40(4) | 50 |
| A4. Explore overlap between Oral Micro and OHS 2 | 60(6) | 10(1) | 70 |
| A5. Reduce the overlap in Oral Micro and Oral Micro & Immunology | 60(6) | 60 | |
| A6. Explore overlap in all above courses and Oral Medicine & Pathology | 30(3) | 30(3) | 60 |
| A7. Remove Oral Micro & Immunology | 10(1) | 40(4) | 50 |
| DHDP Dental Hygiene Theory & Practice (n=10) | |||
| B1. Clinical Considerations | |||
| B.1a: Have consistent hours of clinical time in each term | 30(3) | 30(3) | 60 |
| B.1b: Reduce clinical hours | 20(2) | 10(1) | 30 |
| B2. Move the beginning of community curriculum from Year 2 to Year 1 | 30(3) | 40(4) | 70 |
| B3. Move curriculum from 4th Year Theory & Practice (T&P-4) downwards to 2nd Year Theory & Practice (T&P-2) |
30(3) | 20(2) | 50 |
| B4. Align and synthesize sessions with learning outcomes and time in T&P-1 and T&P-2 | 40(4) | 20(2) | 60 |
| B5. Totally restructure/redesign T&P-4 | 60(6) | 10(1) | 70 |
| B6. Create a new entrepreneurship course from T&P-4 hours | 30(3) | 30(3) | 60 |
Table 3. Summary of round 2 agreement ratings from the perspective of the course content in Research & Epidemiology, Advocacy & Policy and Courses from Non-Dentistry Faculties
| DHDP proposed renewal spaces | Agreement ratings in % with ‘n’ in brackets | ||
|---|---|---|---|
| Agree | Strongly agree | Total | |
| DHDP Research & Epidemiology (n=10) | |||
| C1. Reduce Lit Review 1 and Lit Review 2 to 3 credits | 30(3) | 50(5) | 80 |
| C2. Combine Lit Review 1 and Lit Review 2 into one course | 20(2) | 40(4) | 60 |
| C3. Examine content of Lit Review 1 | 30(3) | 40(4) | 70 |
| C4. Reduce content of Oral Epidemiology | 20(2) | 30(3) | 50 |
| DHDP Advocacy & Policy (n=10) | |||
| D1. Shift Oral Health Care Trends & Topics into Year 1 | 20(2) | 20 | |
| D2. Merge Oral Health Care Trends & Topics content into less sessions | 30(3) | 10(1) | 40 |
| D3. Blending Policy Analysis & Change, Oral Epidemiology and T&P-4 | 10(1) | 10 | |
| Courses from Faculties (n=9) | |||
| E1. Explore overlap in Research & Writing 150, ENGL 110, T&P-1, T&P-2, and Lit Review 1 | 67(6) | 11(1) | 78 |
| E2. Reduce overlap of STAT 203 and Oral Epidemiology | 44(4) | 22(2) | 66 |
| E3. Remove CHEM 121 | 11(1) | 11 | |
| E4. Assess overlap in BIOL 155 and the Biomedical Science courses | 44(4) | 33(3) | 77 |
| E5. Decrease Psychology to 3 credits (currently 6 credits) | 22(2) | 44(4) | 66 |
| E6. Develop a pre-requisite year prior to entry into the DHDP Program | 11(1) | 22(2) | 32 |
Table 4. Summary of round 3 ranking of the most important ideas to implement with 1 being the most important from the perspective of the Biomedical Sciences and Theory & Practice courses
| Suggested renewal spaces | Group ranking data with #1 Being most important (expressed in ‘n’) |
|||
|---|---|---|---|---|
| ‘n’ per | 1 | 2 | 3 | |
| DHDP Biomedical Sciences | ||||
| A1. Explore overlap in Oral Health Sciences 1 (OHS 1) and Oral Health Sciences 2 (OHS 2) | 8 | 3 | 1 | 2 |
| A2. Explore overlap between Oral Micro and OHS 2 | 5 | 1 | 1 | 2 |
| A3. Reduce the overlap in Oral Micro and Oral Micro & Immunology | 7 | 2 | 3 | 1 |
| A4. Explore overlap in all above courses and Oral Medicine & Pathology | 8 | 2 | 2 | 2 |
| DHDP Dental Hygiene Theory & Practice | ||||
| B1. Move the beginning of community curriculum from Year 2 to Year 1 | 8 | 4 | 1 | 1 |
| B2. Move curriculum from 4th Year Theory & Practice (T&P-4) downwards to 2nd Year Theory & Practice (T&P-2) |
5 | 2 | 1 | 1 |
| B3. Align and synthesize sessions with learning outcomes and time in T&P-1 and T&P-2 | 5 | – | 2 | 2 |
| B4. Totally restructure/redesign T&P-4 | 8 | 3 | 3 | 1 |
| B5. Create a new entrepreneurship course from T&P-4 hours | 10 | 2 | 2 | 3 |
Table 5. Summary of round 3 ranking of the most important ideas to implement with 1 being the ‘most important’ from the perspective of course content in Research & Epidemiology, Advocacy & Policy, and Courses from Non-Dentistry Faculties
| Suggested renewal spaces | Group ranking data with #1 Being most important (expressed in ‘n’) |
|||
|---|---|---|---|---|
| ‘n’ per | 1 | 2 | 3 | |
| DHDP Research & Epidemiology Courses | ||||
| C1. Reduce Lit Review 1 and Lit Review 2 to 3 credits | 10 | 3 | 5 | 1 |
| C2. Combine Lit Review 1 and Lit Review 2 into one course | 8 | 5 | 1 | 2 |
| C3. Reduce content of Oral Epidemiology | 6 | 2 | 1 | 2 |
| DHDP Advocacy & Policy Courses | ||||
| D1. Develop new curriculum in public health/advocacy/policy in Year 1 onward | 8 | 7 | 1 | |
| D2. Add into community rotations | 6 | 2 | 2 | 2 |
| D3. Integrate into PBL sessions | 7 | 1 | 3 | |
| D4. Decrease on campus clinical sessions in T&P-1 | 6 | 2 | 1 | |
| Courses from Non-Dentistry Faculties | ||||
| E1. Explore overlap in Research & Writing 150, ENGL 110, T&P-1, T&P-2, and Lit Review 1 | 8 | 5 | 3 | |
| E2. Reduce overlap of STAT 203 and Oral Epidemiology | 9 | 2 | 6 | 1 |
| E3. Assess overlap in BIOL 155 and the Biomedical Science courses | 7 | 1 | 2 | 2 |
| E4. Decrease Psychology to 3 credits | 8 | 2 | 1 | 1 |
The round 2 agreement data have been summarized to identify those with which respondents agreed or strongly agreed. In round 3 items that people did not rank included those with which they disagreed but also those for which they did not feel knowledgeable enough to rank. As one respondent commented: “It is challenging to ‘rank’ courses that we have very limited knowledge about.” While eleven respondents completed round 3, the data for individual items ranged from 4 to 10 responses given the respondents’ knowledge. The ranked data have been summarized to focus on the items that 50% or more of the respondents ranked as first, second, or third.
Respondents indicated that several areas of overlap existed in the biomedical sciences. Overlap in the Oral Health Sciences 1 and 2 course had the highest level of agreement at 80%. However, the overlap between Oral Microbiology and Oral Health Sciences was also rated at 70% agreement as was the overlap in Dental Anatomy and the Head and Neck Anatomy courses <Table 2>. These areas were confirmed in round 3 <Table 4>.
In their written comments, respondents recommended redesigning the courses to make more effective use of instructional time. The following quotes provide some examples.
“Student feedback for many years has indicated repeated learning between Oral Microbiology and Oral Microbiology & Immunology. The course syllabi course contents also point to overlapping areas of learning.”
“Pharmacology also provides a review of microbes, viruses, and fungi related to chemotherapeutic treatments [as does Oral Pathology]”
“Oral oncology is already extensively discussed in Oral Medicine & Pathology.”
These data suggested that the courses within the Biomedical Science section would provide some important opportunities to find renewal spaces.
The courses in the Dental Hygiene Theory & Practice section also identified possible curriculum spaces. One of the highest ratings was given to the shift of community curriculum to Year 1 of the program <Table 2>. The addition of three credits to the first year Theory & Practice course was in the approval process and led to a cascading effect of curriculum moving from Year 4 to Year 1. This allowed for a “total restructure/redesign” of the 4th year
Theory & Practice course as evident in the ranked data <Table 2>. The following quotes provide some context for the ratings.
“The community/public health curriculum can be moved to Year 1 as part of the Dental Hygiene Theory & Practice course, particularly given the focus of UBC’s DHDP on community-engaged learning.”
“Develop new curriculum in public health/advocacy/policy to integrate earlier in the curriculum (Year 1).”
“Introduce the concept [of IPE] in Year 1. If they learned more broadly about the profession of dental hygiene, and how health and dental care are delivered, they may have a less siloed approach to care.”
While this shift was already underway, respondents used the Delphi as an opportunity to confirm its value.
Areas of repeated learning also extended to courses in the Research & Epidemiology section. The highest ratings were given to changing the two literature review courses from four to three credits <Table 3>. The ranked data also showed support for combining the two courses <Table 5>. The following quotes highlight opportunities for curriculum spaces.
“It would be beneficial to ensure Oral Epidemiology starts more harmoniously from where STAT 203 finishes.”
“How is the content of STAT 203 different than the content of Lit Review 1, Lit Review 2 and Oral Epidemiology?”
There were few curriculum spaces identified in the Advocacy & Policy course section <Table 3,5>. Respondents’ comments highlighted additional opportunities to integrate and deepen the Advocacy & Policy curriculum.
“Advocacy and Policy Use – continue building/scaffolding into ‘deeper’ assignments/exposure.”
“Add spiralling of advocacy and policy use into community rotations.”
Respondents supported the importance of the Advocacy & Policy renewal theme.
Many of the first year DHDP courses are implemented through Faculties other than Dentistry with a statistics course also present in 2nd year. The ratings suggested that there were possible areas of repeated learning in many of these courses such as Research & Writing, English, and Biology <Table 3,5>. Analyzing these areas of overlap in the first-year courses with the curriculum in the DHDP program specific course were highly ranked.
Respondents wrote about the value of the courses from the Non-Dentistry Faculties as evident in the following quotes. “Six credits of first-year English requirements are needed to support writing abilities and keeps doors open for further graduate or other advanced study options.”
“Chemistry provides students with a foundation for dental materials and biochemistry if students wish to continue with graduate studies.”
However, there was support <Table 5>. to explore the areas of repeated learning in these courses as evident in the following quotes.
“Exploring is always beneficial, and my understanding is these courses need it.”
“There could be value in assessing overlap of material between BIOL 155 and Oral Microbiology.”
Respondents emphasized the need for more information sharing between the dental hygiene faculty members and those from other Faculties to support effective spiraling of the curriculum.
The idea of spiraling the learning was supported but the amount of repeated learning was also questioned. Faculty members expressed the need for balance.
“Generally, support review of similar courses to reduce overlap and encourage strategic scaffolding as needed.”
“Repeats in a topic area are fine only if the students need a summarizing review before adding or linking to the next area/step of the topic.”
However, there were also words of caution as reflected in the following quotes:
“Do not compromise the foundational knowledge that students will need for the higher-level courses just because we see overlap.”
“The spiraling of the academic writing curriculum from 1st Year … to 4th Year … is sequenced well and facilitates students’ development of writing abilities.”
These data encouraged faculty to analyze how to best layer the learning and assist students in retrieving information from previous courses.
In the open-ended questions, respondents wrote about the challenges with program redesign as reflected from a curriculum perspective.
“Inflexibility’ of an already full academic curriculum schedule to accommodate themes which all demand various degrees of flexibility.”
“Incorporating these additional activities at the expense of other important themes/activities that are required to support graduation (e.g. board exams).”
“Decreasing elasticity in the program -e.g., when do students who are struggling fit in remediation?”
Respondents also discussed challenges such as the increased workload for faculty and the need to have faculty ‘buy in’ at multiple levels as evident below.
“Considerable time is required to ‘modify’ course material to support this realignment.”
“Hiring and/or training of faculty to support these renewal themes.”
“Need ‘buy-in’ from most faculty to support integration of these themes within their own courses/sections.”
“Remaining too territorial over one’s own previously taught curriculum and sessions.”
Based on respondents’ ratings, rankings, and comments, renewal spaces do exist. However, further collaborative decision-making will be essential. As one responded commented: “I would prefer to defer to the course instructors to determine where overlaps exist and how to strengthen learning.”
This Delphi study was embedded within a program redesign phase that was initiated in 2021. The DHDP faculty members and stakeholders had identified three curricular themes that formed the basis for this redesign process including (1) entrepreneurship and leadership, (2) advocacy and policy use, and (3) inter-professional education.
While health sciences literature is rich with recommendations for curriculum development, there are few research-based recommendations to support curriculum renewal [9,12]. The literature directed to program redesign [5,9] suggests that redesign is a more complex process involving more nuanced factors with regard to institutional structures, culture, resources and personnel to name but a few. The Social Entrepreneurship (SE) group asked for ten new 3-hour sessions in the 4th year of the program. The Advocacy & Policy Use group requested eight new 3-hour sessions; this included two new sessions in Year 2, three new sessions in each of Year 3 and Year 4. The Interprofessional Education (IPE) group focused on using the current clinical and community practice hours to integrate new learning experiences; they did not ask for more sessions.
Through the Delphi study a variety of curriculum spaces were found in courses throughout the DHDP <Table 2-5>. In addition to these spaces, several themes about dental hygiene education arose from the data.
Support for the Year 1 introduction of community curriculum including a community experience was highlighted in both the Theory & Practice and the Advocacy & Policy Use sections. This reinforces the view that dental hygiene education needs to acknowledge and emphasize its origin in the public health sector given that the first program established in 1914 was directed to services for children through public health programs [19,20]. Only later did the profession move into the private sector and expand to include preventive and therapeutic services for adults. As one respondent noted: “Do not lose sight of our roots.”
The importance of introducing students to ‘immersive learning experiences’ [21] early in their professional education is emphasized in health professional education [21-23] Early experiences in community environments appear to have a considerable impact on learners [22,23]. They gain an opportunity to see their professional roles through diverse lenses such as advocacy, interprofessional practice, community engagement, and social entrepreneurship [23]. In North America this has traditionally been the focus regarding dental hygiene clinical practice curriculum, but not necessarily community practice. Expanding such immersive experiences to include an introduction to community practice, advocacy and social entrepreneurship in the first year has the potential of revitalizing dental hygiene curriculum.2 It could be started with the integration of self-assessments such as an entrepreneurship self-efficacy instrument.24 The discussions would then need to be continued and advanced as the students move through the program. The potential impact of a minor change could be powerful.
The Delphi data also highlighted both the benefits and the challenges of a spiraling curriculum model. Initially developed in 2007, the DHDP integrated this framework, a concept introduced by Jerome Bruner in 1960. Bruner described the model as a ‘metaphoric spiral’ where teaching begins with fundamental concepts and gradually increases in complexity [25]. This design is particularly evident in the large DHDP umbrella courses such as Dental Hygiene Theory and Practice and Oral Health Sciences.
A spiral curriculum involves the ‘iterative revisiting’ [25-28] of topics, subjects and/or themes throughout the program. It involves a deepening of the subject matter with each new encounter building on previous ones. It involves (a) re-examining subjects/themes, (b) advancing to greater degrees of difficulty, (c) developing new connections, and (d) continuing deepening of knowledge and abilities leading to increased competency. It has been found to increase students’ knowledge base in the basic sciences when compared to the more traditional disciple-based courses [26]. Advocates suggest a spiral curriculum supports ‘horizontal integration’ to break down the subject silos common in discipline-based courses [28].
In a study by Coelho and Moles [27], dental students indicated that they appreciated the opportunities to consolidate information and revisit information to deepen their learning. However, first year students described a spiral curriculum to be more challenging; it was found to be ‘uncomfortable’ and ‘uncertain.’ The authors suggest these adjectives may reflect the views of students who have succeeded with a ‘cram and dump’ approach. However, senior students expressed a greater appreciation for the spiral curriculum.
It is important not to underestimate the challenges students may face when engaging with a spiral curriculum [26-28]. Ireland and Mouthaan [28] suggest that students who make the connections easily, find the spiraling aspects repetitive and unnecessary, while others struggle and can easily be left behind. However, this is likely not unique to a spiraling curriculum framework. Davis and Harden [26] emphasized the need for a clear interface between each ‘phase’ or ‘loop’ of the spiral. To support students in transitioning to more complex levels, they introduced a dedicated course; however, the scope of this course was not specified. From the perspective of the DHDP, offering a session at the beginning of each term, outlining the term’s learning outcomes in relation to the program’s graduate outcomes, could help students better grasp the increasing expectations for critical thinking and analysis.
The Delphi textual data suggest that increased curriculum integration would be beneficial for the DHDP. Fragmented, piecemeal curriculum revisions may have diminished the clarity of the original spiral design. Significant areas of repeated learning also likely stem from limited resources, including limited faculty time to analyze and further shape the spiral curriculum. This issue is especially evident in courses from other disciplines. The curriculum has to indeed spiral; learned material cannot just be a repetition. Layers of complexity need to be added when revisiting topics and themes [27]. The respondents emphasized the need for such a balance in the spiraling process.
Studies [5,9,29] including ours highlight the critical need for ongoing curriculum renewal. The DHDP has well-established channels through which students and faculty provide input about the curriculum. However, respondents noted recurring feedback from students over several years about areas of perceived repetition of curriculum. Such feedback reflects the challenges inherent in redesign efforts; such efforts require faculty resources.
Redesign efforts must account for institutional structures, culture, and limitation in resources [5,30]. There is a need for time to address the dynamic personnel forces at work [5]. Delphi respondents identified faculty members perceived ownership of particular curriculum could be a deterrent for change. Newell et al [29] support the position that redesigning curriculum may often be perceived as a negative critique of current course content, and faculty members may feel a loss of curricular control. Course changes frequently impact the professional identities of faculty members. Redesign efforts involve risks and uncertainties for faculty members and can, therefore, be stressful. Becker [5] highlights the importance of fostering collective ownership of courses within the program. Finding more time for faculty members across disciplines to assess the spiraling curriculum could assist in supporting a collective program ownership in the DHDP.
Harden [30] further proposed that curriculum integration exists on a continuum, visualized as an ‘integration ladder’ with eleven steps, ranging from ‘isolation’ to ‘trans-disciplinary’ design. Lower steps emphasize sharing of information and resources among faculty. The higher steps involve more coordinated planning where faculty collaborate on the development of layered curriculum themes such as oral pathology. At that level, the curriculum incorporates interdisciplinary and multidisciplinary strategies in curriculum implementation. It appears that some DHDP courses are at the lower rung level of ‘awareness’ and in other areas at the top rung of ‘multi-disciplinary.’ With regard to the basic science courses, more opportunities to collaboratively explore the curriculum would be beneficial for faculty and students alike.
Twenty-six hours across 13 sessions were made available to implement social entrepreneurship curriculum into the 4th year DHDP Dental Hygiene Theory & Practice course. However, there is ongoing discussion about integrating social entrepreneurship into first year to allow learners to reflect on entrepreneurship as they engage in their community experiences throughout the program.
The 24 hours requested for advocacy are currently being threaded throughout the four years of the DHDP to support the development of such abilities in all terms of the DHDP. Changes are also underway to increase the intra-professional collaboration experiences with the dental students in various areas, including the first-year community experience. The intention is to keep strengthening and augmenting the interprofessional curriculum. Revisions have also been made in the biological science courses. The sequence of learning in such areas as head and neck anatomy, tooth development, and dietary counselling have been shaped to promote increased depth of learning. Faculty members are working through the various study recommendations to support more effective spiraling of the curriculum.
The response rate varied over the 3 rounds of the study, with the first round including the highest number of respondents (n=13; 81%); this resulted in the generation of diverse ideas for consideration. Round 2 included the lowest response rate (n=9; 56%) and the response rate then increased in round 3 (n=11; 69%). Such attrition is common in studies that involve several rounds of participation. Despite the attrition, the majority of course coordinators participated and diversity of expertise was still present throughout the rounds <Table 1>. While the respondents were selected for their content expertise and knowledge of the DHDP curriculum, that knowledge did not extend to all the courses within the program. Respondents appeared to be more comfortable in rating suggestions related to their own subject familiarity, but less willing to rank other items. Their knowledge base likely affected their response rate but did not necessarily affect the quality of the data. They likely did not wish to dilute the data by submitting less informed opinions. The overall response rate was supportive for making informed curriculum decision.
The findings of this study are specific to the UBC program. However, the curriculum spaces found, and the issues encountered in the redesign process are expected to be relevant for faculty across the health professions.
This Delphi study was embedded within a UBC dental hygiene program redesign phase that was initiated in 2021 and completed in 2022. The faculty members and stakeholders had identified new curricular themes and curriculum spaces needed to be found within the existing program. The Delphi approach provided an anonymous approach to gain consensus on the curriculum spaces present in the program.
Key findings from this study highlight:
The importance of honouring the history of the dental hygiene profession, particularly through the early introduction of community practice before the onset of clinical experiences.
The inherent challenges of redesigning a program when compared to creating a new program given faculty members may experience a sense of loss of their expertise.
The value of periodic comprehensive program reviews to address curriculum imbalances that can occur over time by piecemeal course revisions.
The commitment of faculty members to find spaces for the renewal themes focused on advocacy, policy use, social entrepreneurship and interprofessional education.
The need to create ongoing communication channels for program faculty and faculty members from other departments to connect about their ever evolving curriculum areas. While faculty members commonly have such channels within their program, they often have few channels to communicate with those from other areas.
While the findings are specific to the UBC’s DHDP, the Delphi methodology supported the identification of key findings related to the sequencing of community curriculum, the challenges of spiraling curriculum, the redesign process as well as curriculum areas in which spaces could conceivably be found. These are likely to resonate with faculty across the oral health professions in Canada and internationally. The Delphi approach provides rich data for program redesign and renewal that others could apply to their program curriculum.
Both authors participated in the design of the study, the ongoing analysis of the data, and the writing of the manuscript.
The authors declared no conflicts of interest.
This study was funded through the University of British Columbia (UBC), Canada, through an Advancing Education Renewal Grant.
This study was approved by the University of British Columbia (UBC), Office of Research Ethics (H21-02608).
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
The authors wish to acknowledge the ongoing input of the other members of the DHDP Curriculum Renewal Task Force including R Carvalho, L Donnelly, DM Laronde, K Hiemstra, H Kilian, N Shafiq, and E Whitney as well as the research assistant, S. Kaytal.
Canadian Dental Hygienists Association (CDHA). Canadian competencies for dental hygiene programs [Internet]. Ottawa (ON): CDHA; 2015 [cited 2021 Nov 04]. Available from: https://doi.files.cdha.ca/profession/CCBDHP_report.pdf.
Sunell S, Hatzimanolakis P, Dhami C, Shariati B, Rhodes-Nesset S, Kanji, et al. Developing a social entrepreneurship curriculum for baccalaureate dental hygiene education. Int J Dent Hyg. 2025 [in press].
Sunell S, Laronde DM, Kanji Z. Dental hygiene graduates’ educational preparedness: self-confidence ratings of the CDHA baccalaureate competencies. Int J Dent Hyg. 2020;18(3):295-306. https://doi.org/10.1111/idh.12434.
Sunell S, Laronde DM, Kanji Z. 4th Year dental hygiene students’ educational preparedness: self-confidence ratings of the CDHA Baccalaureate Competencies (2017-2019). J Dent Educ. 2021;85(6):768-77. https://doi.org/10.1002/jdd.12546.
Becker TB. Redesign and process of reforming an existing undergraduate nutritional sciences program. Adv Physiol Educ. 2020;44(4):570-8. https://doi.org/10.1152/advan.00029.2020.
McLean. Educational expansion or credential Inflation? The evolution of part-time study by adults at McGill University, Canada. Int J Lifelong Educ. 2010;29(6):739-55. https://doi.org/10.1080/02601370.2010.523944.
Lehmann W. Extra-credential experiences and social closure: working-class students at university. Br Educ Res J. 2012;38(2):203-18. https://doi.org/10.1080/01411926.2010.535894.
Kariya T. Credential inflation and employment in ‘universal’ higher education: enrolment, expansion and (in)equity via privatisation in Japan. J Educ Work. 2011;24(1/2):69-94. https://doi.org/10.1080/13639080.2010.534444.
Lai S, Buchheit BM, Kitamura K, Cook MR, Yarris LM, Chen G, et al. Five key articles on curriculum development for graduate medical educators. J Grad Med Educ. 2024;16(1):75-9. https://doi.org/10.4300/JGME-D-23-00208.1.
Chalupa RL. Using kern’s model to redesign a postgraduate curriculum for orthopaedic physician assistants. J Physician Assist Educ. 2023;34(1):54-7. https://doi.org/10.1097/JPA.0000000000000478.
Chen BY, Kern DE, Kearns RM, Thomas PA, Hughes MT, Tackett S. From modules to MOOCs: application of the six-step approach to online curriculum development for medical education. Acad Med. 2019;94(5):678-85. https://doi.org/10.1097/ACM.0000000000002580.
Mcleod P, Steinert Y. Twelve tips for curriculum renewal. Med Teach. 2015;37(3):232-8. https://doi.org/10.3109/0142159X.2014.932898.
Best L, Walton JN, Walker J, von Bergmann HC. Reaching consensus on essential biomedical science learning objectives in a dental curriculum. J Dent Educ. 2016;80(4):422-9. https://doi.org/10.1002/j.0022-0337.2016.80.4.tb06100.x.
De Luca E, Sena B, Cataldi S, Fusillo F. Delphi survey of health education system and interprofessional nurse’ role. Nurse Edu Today. 2021;99:104779. https://doi.org/10.1016/j.nedt.2021.104779.
Yang J, Liu Y, Wei W, Xia S, Tang X, Wu L, et al. Delphi study to evaluate competency comprehensive assessment system for professional degree of dentistry. J Dent Educ. 2025;89(9):1386-94. https://doi.org/10.1002/jdd.13864.
Dera AH. Curriculum mapping and alignment of the neuroscience block in an undergraduate medical education program: a Delphi study. Adv Med Educ Pract. 2021;12:567-75. https://doi.org/10.2147/AMEP.S263915.
Timmerberg JF, Dole R, Silberman N, Goffar SL, Mathur D, Miller A, et al. Physical therapist student readiness for entrance into the first fulltime clinical experience: a Delphi study. Phys Ther. 2019;99(2):131-46. https://doi.org/10.1093/ptj/pzy134.
Humphrey-Murto S, Wood TJ, Varpio L. When I say… consensus group method. Med Educ. 2017;51(10):994-5. https://doi.org/10.1111/medu.13263.
Cramer CK, Klasser GD, Epstein JB, Sheps SB. The Delphi process in dental research. J Evid Based Dent Pract. 2008;8(4):211-20. https://doi.org/10.1016/j.jebdp.2008.09.002.
Kanji Z, Sunell S, Boschma G, Imai P, Craig BJ. A discourse on dental hygiene education in Canada. Int J Dent Hyg. 2011;9(4):242–9. https://doi.org/10.1111/j.1601-5037.2010.00495.x.
Marzo-Navarro M, Berné-Manero C. Analysing cross-cutting competencies learning in an online entrepreneurship context. Educ Inf Technol. 2023;28(5):5551-65. (EJ1377579). https://doi.org/10.1007/s10639-022-11359-z.
Afeli SA. Curriculum content for innovation and entrepreneurship education in US pharmacy programs. Ind High Educ. 2022;36(1):13-8. https://doi.org/10.1177/0950422220986314.
Backes DS, Colomé JS, Mello GB, Gomes RCC, Lomba MLLF, Ferreira CLL. Social entrepreneurship in the professional training in Nursing. Rev Bras Enferm. 2022;75(3):e20220391. https://doi.org/10.1590/0034-7167-2021-0391.
Mollica AG, Cain K, Callan RS. Using assessments of dental students’ entrepreneurial self-efficacy to aid practice management education. J Dent Educ. 2017;81(6):726-31. https://doi.org/10.21815/JDE.016.036.
Harden RM, Stamper N. What is a spiral curriculum? Med Teach. 1999;21(2):141-3. https://doi.org/10.1080/01421599979752.
Davis MH, Harden RM. Planning and implementing an undergraduate medical curriculum: the lessons learned. Med Teach. 2003;25(6):596608. https://doi.org/10.1080/0142159032000144383.
Coelho CS, Moles DR. Student perceptions of a spiral curriculum. Eur J Dent Educ. 2016;20(3):161-6. https://doi.org/10.1111/eje.12156.
Ireland J, Mouthaan M. Perspectives on curriculum design: comparing the spiral and the network models. Res Matters. 2020;30:7-12. https://doi.org/10.17863/CAM.100405.
Newell A, Foldes CA, Haddock AJ, Ismail N, Moreno NP. Twelve tips for using the understanding by design curriculum planning framework. Med Teach. 2024;46(1):34-9. https://doi.org/10.1080/0142159X.2023.2224498.
Harden RM. The integration ladder: a tool for curriculum planning and evaluation. Med Educ. 2000;34(7):551-7. https://doi.org/10.1046/j.1365-2923.2000.00697.x.