
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Hye-Won Choi![]() , Do-Seon Lim
, Do-Seon Lim![]() , Hee-Jung Lim
, Hee-Jung Lim![]() , Im-Hee Jung
, Im-Hee Jung![]()
Department of Dental Hygiene, Graduate School of Health Science, Eulji university
Correspondence to Im-Hee Jung, Department of Dental Hygiene, Eulji University, 553 Sanseong-daero, Sujeong-gu, Seongnam-si, Gyeonggi-do, 13135, Korea. Tel: +82-31-740-7247, Fax: +82-31-740-7352, E-mail: Jungih@eulji.ac.kr
Volume 25, Number 6, Pages 487-97, December 2025.
J Korean Soc Dent Hyg 2025;25(6):487-97. https://doi.org/10.13065/jksdh.2025.25.6.3
Received on November 03, 2025, Revised on November 27, 2025, Accepted on December 01, 2025, Published on December 30, 2025.
Copyright © 2025 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objective: Interprofessional education (IPE) promotes effective collaboration among healthcare professionals and has been increasingly implemented in Korea. And a Korean-style IPE assessment tool was recently developed but has not been implemented in practice. Therefore, this study applied the newly developed assessment tool to real-life educational settings to evaluate its effectiveness. Methods: Seven university departments participated in the IPE course. A total of 62 students and seven professors used the IPE assessment tool, which was developed in a previous study, to evaluate the core IPE competencies, before and after the program. Results: After the IPE course, the scores increased from 4.5 to 4.7 in the learning stage and from 4.4 to 4.7 in the behavior stage. Subsequent stage scores were also high: 4.7 in the reaction stage, 4.6 in the professor result stage, and 4.8 in the team member result stage. In the learning stage, ‘Values/ethics for inter-professional practic’ and ‘Roles/responsibilities,’ significantly increased, and in the behavior stage, all competencies significantly increased. Learning, behavior, and reaction stages were positively correlated, as were the four core competencies, with moderate-to-high correlations. Conclusions: In this study, a newly developed Korean-style IPE assessment tool was evaluated, and it was confirmed that the IPE program at the target university significantly improved the core competencies of participating students in the learning and action stages.
Clinical competence, Co-operative behavior, Educational measurement, Inter-disciplinary communication, Inter-professional education
Interprofessional education (IPE) is a vital educational approach that enables healthcare professionals to work together more effectively by learning from and about each other [1]. Gaining increasing attention in the healthcare field, this educational method allows healthcare professionals to understand each other’s work and learn how to collaborate more effectively [1]. A study by Hammick et al. [2] found that students who received IPE were more effective in clinical collaboration. Another study by D’Amour and Oandasan [3] reported that healthcare professionals engaged in clinical practice who received IPE were able to better understand each other’s roles, thus improving their teamwork, communication and collaboration skills. Accordingly, the World Health Organization (WHO) has recommended that healthcare students implement IPE to foster collaborative relationships in the future [4]. In addition, the Interprofessional Education Collaborative (IPEC) was established in the United States in 2009 by six healthcare-related education associations to promote active learning. IPEC defined four core competencies for IPE (‘Values/ethics for interprofessional practice,’ ‘Roles/responsibillities,’ ‘Interprofessional communication,’ ‘Teams and teamwork’) and proposed their integration into curricula [5].
In fact, since 1994, the University of Maryland in the United States has provided an interdisciplinary, team-based, integrated education project for students majoring in various health fields, focusing on the treatment and care of elderly patients [6]. In 2001, the College of Health Disciplines at the University of British Columbia (UBC) in Canada was established and began offering IPE to healthcare students [7]. Some universities in Korea are also implementing IPE. Examples include the ‘WHO integrated health education program’[8], which provided education on team-based treatment methods, and the ‘Interprofessional linkage education program’[9], which operated under the theme of interdisciplinary linkage and collaboration among students from five health care fields.
As IPE has become established in the Korean curriculum, as well as abroad, there has been a need for tools to evaluate interprofessional competencies according to domestic circumstances [10]. The following scales have been developed: the Readiness for Interprofessional Learning Scale (RIPLS) [11], the Interdisciplinary Education Perceptions Scale (IEPS) [12], the Self-efficacy for Interprofessional Experimental Learning Scale (SEIEL) [13], and the Interprofessional Attitudes Scale (IPAS) [14]. However, these tools have limitations in that they cannot assess core competencies, focusing instead on attitudes and perceptions [14,15]. Accordingly, a new assessment tool has recently been developed to address these limitations and fit Korean circumstances [16]. This assessment tool can evaluate the four core competencies of IPE directly. Using the ‘Kirkpatrick assessment model’ enables a thorough evaluation of the entire educational process, including learners’ knowledge and behavioural changes, outcomes and satisfaction. Furthermore, as a tool designed specifically for the Korean context, it has been translated and adapted for use at each educational stage. This effectively reflects the subtle nuances of the language, reducing potential confusion caused by a foreign language and enabling Korean users to conduct more accurate assessments. This study therefore aimed to apply the newly developed assessment tool to actual education, evaluating educational effectiveness among learners and instructors at a university implementing IPE.
This study was conducted with ethical approval (No. EU22-61) from the Institutional Review Board (IRB) at Eulji University. This study targeted a multi-professional education program at a university in Gyeonggi Province that was implementing IPE. Prior consent was obtained from both the professors running the program and the students enrolled in it before registration. The analysis and evaluation of the participants were intended to include all students (n=70) and professors (n=7) involved in the program (complete enumeration survey). However, some participants requested to withdraw during the study and they were excluded from analysis. Therefore, the final sample comprised 62 students (n=62) and 7 professors (n=7).
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.The overall process of this study is illustrated in <Fig. 1>. This study used the Korean IPE core competency assessment tool developed in a previous study [16], and the evaluation period was set according to the tool’s evaluation structure for each educational stage. Before the start of IPE education, a preliminary evaluation of the student’s IPE core competency level was conducted for each learning stage (2 stages; ‘Learning’ and ‘Behavior’). Afterwards, IPE education was provided and, at the end of the third semester, students evaluated their IPE core competency level for each learning stage (3 stages; ‘Learning,’ ‘Behavior’ and ‘Response’). Additionally, team members and professors evaluated the students’ IPE core competency level (1 stage; ‘Result’), providing an objective third-party perspective.
The IPE program, in which the subjects of this study participated, was developed by a university in Gyeonggi Province to strengthen the collaborative capabilities of healthcare professionals. It is a multidisciplinary, collaborative education program offered to healthcare majors. Offered as a regular elective course within the university, it is open to second- to fourth-year students and consists of three semesters (including summer semesters), each comprising three-hour sessions over 15 weeks. Seven healthcare majors participated in the program, which provides specialized training followed by fieldwork.
Specifically, the first semester covers introductions to IPE, PBL and each specialty, as well as healthcare ethics, interprofessional communication and a basic understanding of the elderly. The second semester focuses on examination, diagnosis, prevention, and management methods for geriatric diseases, as determined by the specialty. In the third semester, students apply their knowledge in real hospitals and clinical settings, interacting directly with patients. By specialty, the department of clinical pathology teaches various clinical pathological examination methods related to the elderly. The Department of Radiology teaches cerebrovascular and electrocardiographic examination methods. The department of physical therapy teaches prevention and management methods for musculoskeletal disorders. The Department of Biomedical Engineering teaches the types and use of musculoskeletal assistive devices. The Department of Nursing teaches examination and management methods for depression and mental illness. The department of dental hygiene teaches examination and management methods for oral diseases prevalent in the elderly. The department of emergency medical services teaches cerebrovascular emergencies and treatment methods.
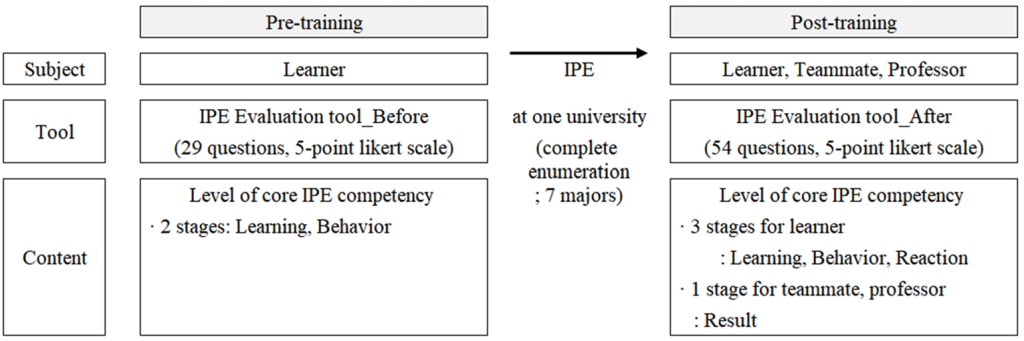
Fig. 1. Experiment procedure
Pre- and post-training evaluations were conducted using the ‘Interprofessional education assessment tool’ [16], which includes four educational stages (learning, behavior, response, and result) and four core competencies (‘Values/ethics for interprofessional practice,’ ‘Roles/responsibillities,’ ‘Interprofessional communication,’ ‘Teams and teamwork’), totaling 29 pre-test items and 54 posttest items <Table 1>; for pre-training <Supplementary material 1> and for post-training <Supplementary material 2>. Items were scored on a 5-point Likert scale (1=not at all, 5=very much). Cronbach’s α demonstrated high reliability across stages (0.840–0.962).
Table 1. Composition of evaluation tool
| Evaluation stage | Subject | Composition | Number of questions | Reliability (Cronbach’s α) | |
|---|---|---|---|---|---|
| Before | After | ||||
| Learning | Learner (n=62) | A. Values/ethics for interprofessional practice | 3 | 3 | 0.930 |
| B. Roles/responsibilities | 4 | 3 | |||
| C. Interprofessional communication | 4 | 4 | |||
| D. Teams and teamwork | 5 | 3 | |||
| Behavior | Learner | A. Values/ethics for interprofessional practice | 2 | 2 | 0.946 |
| B. Roles/responsibilities | 3 | 4 | |||
| C. Interprofessional communication | 5 | 5 | |||
| D. Teams and teamwork | 3 | 4 | |||
| Reaction | Learner | Satisfaction | – | 6 | 0.840 |
| Results | Team member (other learner, n=62) | A. Values/ethics for interprofessional practice | – | 1 | 0.937 |
| B. Roles/responsibilities | 3 | ||||
| C. Interprofessional communication | 3 | ||||
| D. Teams and teamwork | 2 | ||||
| Professor (n=7) | A. Values/ethics for interprofessional practice | – | 1 | 0.962 | |
| B. Roles/responsibilities | 3 | ||||
| C. Interprofessional communication | 4 | ||||
| D. Teams and teamwork | 3 | ||||
| Total number of questions | 29 | 54 | |||
The collected data were statistically analysed using IBM SPSS program (ver. 28.0; IBM Corp., Armonk, NY, USA) at a significance level of 0.05. First, a normality test was performed using the Shapiro-Wilk test, and the data did not conform to a normal distribution. Subsequently, descriptive statistical analysis was performed on the IPE general characteristics and core competency scores by time point and stage. The Mann-Whitney U-test and Kruskal-Wallis test were used to evaluate the degree of improvement in core competencies based on general characteristics. The Wilcoxon rank sum test was used to compare pre- and post-training outcomes. Pearson’s correlation coefficient was used to evaluate the correlation between learning stages and core competencies.
The general characteristics of the study subjects are presented in <Table 2>. Of the 62 students, 74.2% were female and 25.8% male. The most common major was physical therapy (21%), followed by nursing, emergency medical services, radiology, and clinical pathology. Most were in their third year (93.5%). As a result of analyzing the degree of improvement in core competencies (overall average; at learning and behavior stage) before and after training according to general characteristics, no significant differences were observed in any of the items including gender (p=0.118), major (p=0.698), grade (p=0.263), and clinical experience (p=0.092).
<Table 3> shows the average scores of core competencies at each evaluation time and educational stage. All core competencies demonstrated significant improvement from pre- to post-training (p<0.001). Pre-traning scores ranged from 4.2 to 4.7, while posttraining scores exceeded 4.7 across competencies. Notably, ‘A. Values/ethics for interprofessional practice’ and ‘B. Roles/responsibilities’ showed substantial gains during the learning stage, and all competencies increased significantly during the behavior stage.
Table 2. General characteristics of learners
| Characteristics | Division | Number of respondents (N(%)) |
Difference value (Mean±SD) |
p* |
|---|---|---|---|---|
| Gender | Male | 16(25.8) | 0.36±0.31 | 0.118 |
| Female | 46(74.2) | 0.25±0.43 | ||
| Major | Department of physical therapy | 13(21.0) | 0.22±0.09 | 0.698 |
| Department of nursing | 11(17.7) | 0.24±0.42 | ||
| Department of emergency medical services | 10(16.1) | 0.19±0.07 | ||
| Department of radiology | 10(16.1) | 0.15±0.43 | ||
| Department of clinical pathology | 9(14.5) | 0.45±0.54 | ||
| Department of biomedical engineering | 6(9.7) | 0.51±0.48 | ||
| Department of dental hygiene | 3(4.8) | 0.26±0.12 | ||
| Grade | Junior | 58(93.5) | 0.30±0.41 | 0.263 |
| Senior | 4(6.5) | 0.08±0.12 | ||
| Clinical practice | Yes | 27(43.5) | 0.39±0.49 | 0.092 |
| No | 35(56.5) | 0.19±0.29 | ||
| Total | 62(100.0) | 0.28±0.40 |
Difference value represents the gap in average scores for the core competencies before and after the IPE.
*by Mann Whitney U-test, Kruskal-Wallis test or Wilcoxon rank sum test
Table 3. Comparison of core competencies before and after IPE, according to educational stage
| Evaluation stage | Subject | Composition | Core competency | |||
|---|---|---|---|---|---|---|
| Before | After | Z | Cohen’s d | |||
| Learning | Learner | A. Values/ethics for interprofessional practice | 4.52±0.48 | 4.69±0.40* | -2.298 | 0.50765 |
| B. Roles/responsibilities | 4.16±0.63 | 4.75±0.45** | -5.880 | 0.63257 | ||
| C. Interprofessional communication | 4.62±0.40 | 4.69±0.40 | -1.335 | 0.45306 | ||
| D. Teams and teamwork | 4.65±0.37 | 4.74±0.38 | -1.770 | 0.35533 | ||
| Sub-total | 4.50±0.37 | 4.72±0.34** | ||||
| Behavior | Learner | A. Values/ethics for interprofessional practice | 4.30±0.60 | 4.65±0.50** | -3.541 | 0.74071 |
| B. Roles/responsibilities | 4.20±0.73 | 4.71±0.37** | -4.261 | 0.77599 | ||
| C. Interprofessional communication | 4.40±0.50 | 4.69±0.43** | -3.792 | 0.52148 | ||
| D. Teams and teamwork | 4.60±0.48 | 4.74±0.43* | -2.748 | 0.49768 | ||
| Sub-total | 4.38±0.48 | 4.70±0.37** | ||||
| Reaction | Learner | Satisfaction | – | 4.66±0.41 | – | – |
| Results | Team member (other learner) |
A. Values/ethics for interprofessional practice | – | 4.71±0.52 | – | – |
| B. Roles/responsibilities | 4.77±0.45 | |||||
| C. Interprofessional communication | 4.75±0.41 | |||||
| D. Teams and teamwork | 4.77±0.45 | |||||
| Sub-total | 4.76±0.42 | |||||
| Results | Professor | A. Values/ethics for interprofessional practice | – | 4.43±0.54 | – | – |
| B. Roles/responsibilities | 4.71±0.36 | |||||
| C. Interprofessional communication | 4.54±0.39 | |||||
| D. Teams and teamwork | 4.62±0.36 | |||||
| Sub-total | 4.60±0.35 | |||||
| Total | 4.43±0.41 | 4.71±0.34** | ||||
The scores of core competency were written in Mean±SD.
*p<0.05, **p<0.001, by Wilcoxon rank sum test between before and after IPE.
We analyzed the correlations between the educational stages, focusing on the mean post-training scores <Table 4>. Significant moderate to high positive correlations were observed between the learning and behavior stages (r=0.772, p<0.001), learning and reaction stages (r=0.723, p<0.001), and behavior and reaction stages (r=0.826, p<0.001). Other stage correlations were not statistically significant.
Table 4. Correlation by evaluation stage
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Learning learner | 1.000 | ||||
| 2. Behavior learner | 0.826* | 1.000 | |||
| 3. Reaction learner | 0.772* | 0.723* | 1.000 | ||
| 4. Results team member | 0.111 | 0.148 | 0.039 | 1.000 | |
| 5. Results professor | -0.063 | -0.270 | -0.380 | -0.100 | 1.000 |
**p<0.001, by Pearson’s correlation coefficient
Using the average post-training scores, correlations between sub-competencies at each stage were analysed <Table 5>.
Firstly, statistically significant correlations were observed when analysing the relationships between sub-competencies within each stage (p<0.001): the learning stage, the behavior stage and the team-member-targeted result stage. Specifically, in the learning stage, the highest positive correlation was between ‘A. Values/ethics for interprofessional practice’ and ‘C. Interprofessional communication’ (r=0.700). In the behavior stage, ‘C. Interprofessional communication’ and ‘D. Teams and teamwork’ showed the strongest correlation (r=0.774). In the team-member-targeted result stage, the highest positive correlation was observed between ‘C. Interprofessional communication’ and ‘D. Teams and teamwork’ (r=0.903). Meanwhile, in the professor-targeted result stage, strong positive correlations were also observed between ‘A. Values/ethics for interprofessional practice’ and ‘C. Interprofessional communication’ (r=0.906), as well as between ‘C. Interprofessional communication’ and ‘D. Teams and teamwork’ (r=0.906).
Finally, analyses conducted across stages revealed a high positive correlation between ‘D. Teams and teamwork’ in the learning stage and ‘C. Interprofessional communication’ in the behavioral stage (r=0.768, p<0.001). Meanwhile, the competencies of the reaction stage generally showed a high correlation with all competencies within the learning and behavior stages (r=0.511-0.782, p<0.001).
Table 5. Correlation by core competencies after education
| Variables | 1-A | 1-B | 1-C | 1-D | 2-A | 2-B | 2-C | 2-D | 3-A | 4-A | 4-B | 4-C | 4-D | 5-A | 5-B | 5-C | 5-D | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Learning learner | A. Values/ethics for interprofessional practice | 1.000 | ||||||||||||||||
| B. Roles/responsibilities | 0.573** | 1.000 | |||||||||||||||||
| C. Interprofessional communication | 0.700** | 0.689** | 1.000 | ||||||||||||||||
| D. Teams and teamwork | 0.531** | 0.456** | 0.691** | 1.000 | |||||||||||||||
| 2 | Behavior learner | A. Values/ethics for interprofessional practice | 0.524** | 0.332** | 0.652** | 0.712** | 1.000 | ||||||||||||
| B. Roles/responsibilities | 0.521** | 0.445** | 0.689** | 0.607** | 0.708** | 1.000 | |||||||||||||
| C. Interprofessional communication | 0.684** | 0.494** | 0.614** | 0.768** | 0.687** | 0.508** | 1.000 | ||||||||||||
| D. Teams and teamwork | 0.672** | 0.446** | 0.707** | 0.742** | 0.741** | 0.627** | 0.774** | 1.000 | |||||||||||
| 3 | Reaction learner | A. Satisfaction | 0.618** | 0.511** | 0.782** | 0.676** | 0.600** | 0.593** | 0.601** | 0.712** | 1.000 | ||||||||
| 4 | Results team member | A. Values/ethics for interprofessional practice | 0.118 | 0.061 | 0.071 | 0.138 | 0.101 | 0.047 | 0.203 | 0.296* | 0.040 | 1.000 | |||||||
| B. Roles/responsibilities | 0.170 | 0.089 | 0.060 | 0.154 | 0.076 | 0.037 | 0.151 | 0.222 | 0.045 | 0.789** | 1.000 | ||||||||
| C. Interprofessional communication | 0.087 | 0.038 | 0.024 | 0.108 | 0.071 | 0.047 | 0.149 | 0.208 | 0.015 | 0.848** | 0.856** | 1.000 | |||||||
| D. Teams and teamwork | 0.191 | 0.060 | 0.045 | 0.088 | 0.099 | 0.014 | 0.185 | 0.220 | 0.056 | 0.854** | 0.888** | 0.903** | 1.000 | ||||||
| 5 | Results professor | A. Values/ethics for interprofessional practice | 0.000 | 0.204 | 0.189 | 0.091 | 0.354 | 0.387 | 0.213 | 0.314 | 0.427 | 0.283 | 0.033 | 0.241 | 0.283 | 1.000 | |||
| B. Roles/responsibilities | 0.242 | 0.102 | 0.024 | 0.411 | 0.059 | 0.342 | 0.213 | 0.025 | 0.200 | 0.085 | 0.495 | 0.164 | 0.085 | 0.750 | 1.000 | ||||
| C. Interprofessional communication | 0.082 | 0.208 | 0.152 | 0.155 | 0.414 | 0.374 | 0.278 | 0.376 | 0.430 | 0.346 | 0.095 | 0.305 | 0.346 | 0.906** | 0.679 | 1.000 | |||
| D. Teams and teamwork | 0.242 | 0.102 | 0.024 | 0.091 | 0.354 | 0.283 | 0.213 | 0.314 | 0.330 | 0.283 | 0.033 | 0.241 | 0.283 | 0.708 | 0.604 | 0.906** | 1.000 | ||
*p<0.05, **p<0.001, by pearson’s correlation coefficient
Competency-based education focuses on improving learners’ performance based on specific learning objectives [17] and has been shown to minimize the gap between educational settings and clinical practice [18]. Implementing such an approach requires an appropriate tool for assessing competency [19]. Choi et al. [16] recently developed an assessment tool that can directly evaluate the core competencies of IPE. In this study, we applied the tool to a university where IPE was actually implemented, with the expectation that the tool can evaluate the effects of IPE with a focus on core competencies.
To more accurately assess the effectiveness of IPE, this study compared core competency scores before and after training. We observed an increase in scores across all stages and competencies. This finding aligns with Kim et al. [20] investigation of IPE’s effectiveness for healthcare students. In that study, an assessment scale centered on ‘Teams and teamwork,’ ‘Role and responsibility,’ and ‘Communication’ was used, and scores increased after the training. Furthermore, Chua et al. [21] analyzed the learning readiness of medical and nursing students using an assessment tool centered on ‘Teamwork,’ ‘Collaboration,’ and ‘Roles and responsibilities.’ Klugman et al. [22] assessed healthcare students using the ‘Communication skills attitudes scale,’ and found statistically significant increases in scores in these areas after IPE. That is, previous studies have also reported increases in scores in the ‘Role and responsibility,’ ‘Teams and teamwork,’ and ‘Communication’ domains after IPE training. These results are similar to those of the present study. Therefore, while the assessment tool used in this study encompassed all learning stages and core competencies, it is considered useful for evaluating educational effectiveness, similar to existing tools.
During the learning phase, we observed increases in ‘Communication’ and ‘Teams and teamwork’ competencies after the training, but these increases were not statistically significant. This is likely because the university in question was operating IPE for third- and fourth-year students capable of integrative thinking across all areas, which likely contributed to their already high level of competency prior to the training. A previous study [23] analyzed differences in communication competency levels across grade levels and reported that third-year students had significantly higher average scores in communication skills compared to first-year students. Furthermore, Kim [24], who examined differences in collaboration skills by grade level, reported that average scores for collaboration skills increased with increasing grade level. This suggests that communication and collaboration skills improve with increasing grade level. In other words, because the participants in this study were seniors, their communication and team collaboration scores were probably higher before the training, which likely explains the insignificant increase in scores before and after the training. Nevertheless, the slight increase in post-training scores demonstrates that IPE was effective in enhancing communication and team collaboration skills.
Furthermore, a correlation analysis was conducted to examine the relationships between the stages. The results revealed moderate to high positive correlations between the learning and behavior stages, the learning and response stages, and the behavior and response stages. All of these correlations were statistically significant. These findings are similar to those of Park [25] and Liebermann and Hoffmann [26], who also used the Kirkpatrick model to identify the impact of service education on performance. However, unlike previous studies, this study did not identify significant correlations between the learning and outcome stages, or between the action and outcome stages. This is likely due to the fact that the evaluators of the result stage differed from those of the learning and behavior stages. The evaluators of the result stage were professors and team members. The evaluators of the learning and behavior stages were different because they were implemented through self-assessment. Consequently, no significant relationships were found between the learning and result stages, or between the behavior and result stages. According to a study by Kim et al. [27], who evaluated problem-centered learning by categorizing subjects as professors, team members, or self-evaluators, there may not be a significant correlation between professor and self-evaluations, or between team member and self-evaluations. This was attributed to differences in expertise and objectivity among the evaluators.
Meanwhile, a correlation analysis conducted between core competencies also confirmed a moderate to high level of positive correlation. A previous study examining the relationship between competencies found that when team members’ needs for recognition and mutual respect are met, it facilitates interaction and leads to cooperative behavior. In other words, when team members feel respected, they naturally engage in cooperative behavior. Seo’s study [29] also argued that systematic collaboration among professionals from various fields is essential for integrated therapy, and that understanding each field’s role, sharing information, and actively communicating play crucial roles. Therefore, sharing information about one’s own field and actively communicating can foster team cooperation. Furthermore, Chung’s study [30] found that communicating while acknowledging others as individuals fosters respect for others and cooperation. Thus, the four core competencies of IPE are closely intertwined and inextricably linked. This study also confirmed moderate to high quantitative correlations between these competencies. In particular, the highest correlation coefficients were observed between ‘Communication’ and ‘Teams and teamwork’, which is consistent with the results of a prior study [30]. In other words, the organic relationships among the core competencies presented in IPEC were confirmed. Therefore, rather than categorizing them by competency, we recommend providing IPE by organically linking all core competencies organically.
Although this study was conducted as a complete enumeration, it focused on a single university and the learners’ majors were not evenly distributed. The fact that the focus was on upperclassmen may also have influenced the results. Therefore, future research requires more precise subject selection and a larger sample size. Nevertheless, this study is significant because it directly applied a recently developed assessment tool to IPE practice and verified its effectiveness. It is hoped that these results will be useful for future interdisciplinary education initiatives.
This study aimed to apply a recently developed assessment tool to participants in interdisciplinary education and further explore its applicability. To this end, evaluations were conducted using the tool with all students and professors of IPE courses offered at a single university in Korea. The results are as follows:
1. Following the training, the average self-assessment score for each competency was approximately 4.7 out of 5, which is a statistically significant increase compared to pre-training scores. In particular, statistically significant differences were observed in the ‘Values/ethics for interprofessional practice’ and ‘Role and responsibility’ competencies during the learning stage, and in all competencies during the behavior stage. Furthermore, the average scores for each competency, as assessed by professors and team members, were also high, exceeded 4 points, confirming that IPE can effectively enhance learners’ competencies.
2. Analysis across the learning stages revealed statistically significant positive correlations between the learning, behaviour and response stages. Analysis across sub-competencies revealed statistically significant positive correlations in all sub-competencies in the learning, behaviour and team-member-targeted result stages. Specifically, the highest correlations were observed between the ‘Role and responsibility’ and ‘Communication’ competencies, as well as between ‘Communication’ and ‘Teams and teamwork.’ In the professor-targeted result stage, meanwhile, statistically significant positive correlations were observed between the ‘Values/ ethics for Interprofessional Practice’ and ‘Communication’ competencies, as well as between the ‘Communication’ and ‘Teams and Teamwork.’
This study reaffirmed the effectiveness of interdisciplinary education in enhancing the core competencies of participating students. We hope these results will contribute to the efficient operation and improvement in quality of future interdisciplinary education.
Conceptualization: IH Jung, HW Choi; Data collection: HW Choi; Formal analysis: HW Choi; Writing-original draft: HW Choi; Writing-review&editing: HW Choi, DS Lim, HJ Lim, IH Jung
The authors declared no conflicts of interest.
None.
This study was approved by the Institutional Review Board (IRB) of Eulji University (IRB No. EU22-61).
Data can be obtained from the corresponding author.
None.
Lee HK, Kim IS, Kim GS, Kim JH, Lee TW, Lee KH, et al. Differences between perceived readiness for interprofessional learning in nursing and other health-related students. J Korean Acad Soc Nurs Educ 2019;25(3):312-20. http://doi.org/10.5977/jkasne.2019.25.3.312.
Hammick M, Freeth D, Koppel I, Reeves S, Barr H. A best evidence systematic review of Interprofessional education. Med Teach 2007;29(8):735-51. https://doi.org/10.1080/01421590701682576.
D’amour D, Oandasan I. Interprofessionality as the field of interprofessional practice and interprofessional education: an emerging concept. J Interprof Care 2005;19(1):8-20. https://doi.org/10.1080/13561820500081604.
World Health Organization. WHO patient safety curriculum guide: multi-professional edition 2011. Swiss: World Health Organization; 2011: 25-7.
Oandasan I, Reeves S. Key elements for interprofessional education. Part 1: the learner, the educator and the learning context. J Interprof Care 2005;19(S1):21-38. https://doi.org/10.1080/13561820500083550.
University of Maryland Baltimore. An age-friendly university [Internet]. University of Maryland Baltimore [cited 2023 Jun 03]. Available from: https://www.umaryland.edu/ggear/.
Yoon BJ, Lee JH. A review study on interprofessional college education in health care sector. J Korean Soc Sch Health 2010;11(1):149-58.
Gumi University. GU-IHEC [Internet]. Gumi University [cited 2023 Jun 08]. Available from: https://www.gumi.ac.kr/pages/sub.htm?nav_code=gum1682324156&code=&Keywords=GU-IHEC.
Gwangju Health University. Korean interprofessional practice&education network [Internet]. Gwangju Health University [cited 2023 Jun 08]. Available from: https://search.ghu.ac.kr/front/Search.jsp.
Remington TL, Foulk MA, Williams BC. Evaluation of evidence for interprofessional education. Am J Pharm Educ 2006;70(3):66. https://doi.org/10.5688/aj700366.
Parsell G, Bligh J. The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Medical Education 1999;33(2):95-100. https://doi.org/10.1046/j.1365-2923.1999.00298.x.
Luecht RM, Madsen MK, Taugher MP, Petterson BJ. Assessing professional perceptions: design and validation of an Interdisciplinary Education Perception Scale. J Allied Health 1990;19(2):181-91.
Mann K, McFetridge-Durdle J, Breau L, Clovis J, Martin-Misener R, Matheson T. Development of a scale to measure health professions students’ self-efficacy beliefs in interprofessional learning. J Interprof Care 2012;26(2):92-9. https://doi.org/10.3109/13561820.2011.640759.
Norris J, Carpenter JG, Eaton J, Guo JW, Lassche M, Pett M, et al. The development and validation of the interprofessional attitudes scale: assessing the interprofessional attitudes of students in the health professions. Acad Med 2015;90(10):1394-400. https://doi.org/10.1097/ACM.0000000000000764.
Gillan C, Lovrics E, Halpern E, Wiljer D, Harnett N. The evaluation of learner outcomes in interprofessional continuing education: a literature review and an analysis of survey instruments. Med Teach 2011;33(9):461-70. https://doi.org/10.3109/0142159X.2011.587915.
Choi HY, Lim HJ, Kim MC, Lim DS, Hwang YS, Jung IH. Development of an interprofessional education evaluation tool. J Korean Soc Dent Hyg 2023;23(4):277-86. https://doi.org/10.13065/jksdh.20230031.
Pijl-Zieber EM, Barton S, Konkin J, Awosoga O, Caine V. Competence and competency-based nursing education: finding our way through the issues. Nurse Educ Today 2014;34(5):676-8. https://doi.org/10.1016/j.nedt.2013.09.007.
Applin H, Williams B, Day R, Buro K. A comparison of competencies between problem-based learning and non-problem-based graduate nurses. Nurse Educ Today 2011;31(2):129-34. https://doi.org/10.1016/j.nedt.2010.05.003.
Morris MC, Gallagher TK, Ridgway PF. Tools used to assess medical students competence in procedural skills at the end of a primary medical degree: a systematic review. Med Educ Online 2012;17:18398. https://doi.org/10.3402/meo.v17i0.18398.
Kim YJ, Radloff JC, Stokes CK, Lysaght CR. Interprofessional education for health science students’ attitudes and readiness to work interprofessionally: a prospective cohort study. Braz J Phys Ther 2019;23(4):337-45. https://doi.org/10.1016/j.bjpt.2018.09.003.
Chua AZ, Lo DY, Ho WH, Koh YQ, Lim DS, Tam JK, et al. The effectiveness of a shared conference experience in improving undergraduate medical and nursing students’ attitudes towards interprofessional education in an Asian country: a before and after study. BMC Med Educ 2015;15(1):233. https://doi.org/10.1186/s12909-015-0509-9.
Klugman CM, Peel J, Beckmann-Mendez D. Art rounds: teaching interprofessional students visual thinking strategies at one school. Acad Med 2011;86(10):1266-71. https://doi.org/10.1097/ACM.0b013e31822c1427.
Baek PG. A study on the relationships and characteristics between Korean collegiate essential skills and undergraduates’ individual variant factors. Korean J Gen Educ 2013;7(3):349-87.
Kim SJ. A study on the difference of collaboration ability according to collaboration experience and collaboration recognition among college students. Korean J Gen Educ 2019;13(3):53-75.
Park YJ. A study on measuring the educational effects of service training program in call center: focused on Kirkpatrick model. Journal of Corporation and Innovation 2019;42(2):65-87. https://doi.org/10.22778/jci.2019.42.2.65.
Liebermann S, Hoffmann S. The impact of practical relevance on training transfer: evidence from a service quality training program for German bank clerks. International Journal of Training and Development 2008;12(2):74-86. https://doi.org/10.1111/j.1468-2419.2008.00296.x.
Jung EJ, Sung S, Woo SM. HRD practitioners’ recognition of the Kirkpatrick evaluation model: focused on strengths, limits, and improvements. KJHRDQ 2016;18(3):115-43. https://doi.org/10.18211/kjhrdq.2016.18.3.005.
Kim HS, Park DH. Lee JH. The effects of store managers’ empowering leadership on contact employees’s cooperative behavior: The mediating role of team trust and the moderating role of team cynicism. Korean J Ind Organ Psychol 2015;28(1):23-60. https://doi.org/10.24230/kjiop.v28i1.23-60.
Seo BS. The needs of therapists on therapeutic support for young children with developmental delays: with a special reference to the child day care center [Master’s thesis]. Yongin: Dankook University, 2012.
Chung HS. Direction of the Korean language education curriculum in the era of SMART education —Based on the principles of respect for human life and cooperation of language and communication—. Korean Lang Educ Res 2014;49(1):5-49. https://doi.org/10.20880/kler.2014.49.1.5.