
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Yu-Na Han1![]() , Kyung-Seok Hu2
, Kyung-Seok Hu2![]()
1Department of Dentistry, The Graduate School, Yonsei University
2Division in Anatomy & Developmental Biology, Department of Oral Biology, College of Dentistry, Yonsei University
Correspondence to Kyung-Seok Hu, Division in Anatomy & Developmental Biology, Department of Oral Biology, Yonsei University College of Dentistry, 50-1 Yonsei-ro, Seodaemun-gu, Seoul-si, 03722, Korea. Tel: +82-2-2228-3047, E-mail: hks318@yuhs.ac
Volume 25, Number 6, Pages 499-508, December 2025.
J Korean Soc Dent Hyg 2025;25(6):499-508. https://doi.org/10.13065/jksdh.2025.25.6.4
Received on August 21, 2025, Revised on October 31, 2025, Accepted on November 27, 2025, Published on December 30, 2025.
Copyright © 2025 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: This study aimed to determine the depth of the facial artery from the skin to prevent complications related to noninvasive surgery and minimal invasive diagnosis. Methods: Forty volunteers (23 males and 17 females) were include in this study. Sonographic images were obtained horizontally. Three surface anatomical landmarks were used: the as antegonial notch (F1), 1 cm lateral to thecheilion (F3), and the nasal alare (F5). Two additional reference points were added at the midpoints between F1 and F3 (F2), and between F3 and F5 (F4). Results: The facial artery was observed at every fifth landmark in 40 cases. The depth of the facial artery was 9.3±2.2 mm at F1, 8.8±3.0 mm at F2, 6.9±3.5 mm at F3, 4.8±1.4 mm at F4, and 5.0±1.6 mm at F5. Conclusions: Further improvements to this study will provide additional data for the medical field. If a clinic has an ultrasound machine the structure should be evaluated by ultrasound before the procedure.
Arterial depth, Facial artery, Non-invasive, Sonography, Venous anatomy
The facial artery starts splitting from the external carotid artery and goes up towards the face, winds around mandibular angle anterior notch, and travels upwards through the anterior margin of the masseter muscle towards the nasion or glabella [1]. The facial artery branch is divided into lateral nasal branch, angular branch, and facial artery ends symmetrically [2]. Facial artery is placed not too deep from the surface of the skin. When penetrating or pressing the facial artery during non-invasive surgery or minimal invasive surgery, a high risk of serious complications and side effects might be entailed which calls for precautions of avoiding the anatomical location of the facial artery. The facial artery was located lateral to the ala of the nose and lateral to the oral commissure [3]. The nasolabial region has an abundant blood supply, which is provided mainly by the facial artery [2]. Ultrasound devices have been developed recently, and the use of them has increased gradually as they are increasingly used in the medical and dentistry fields. The ultrasound diagnosis was performed mainly by a radiologist in former times, thereby limiting the treatments utilizing ultrasound to a particular area only.
However, clinician has a good knowledge of anatomy, ultrasound diagnosis can be utilized directly by the clinician to combine the findings of the lesion, diagnosis, and post-operations without difficulty by mastering the use of ultrasound diagnosis within a short period of time [4]. With respect to observable structures: cautious interpretation is necessary in viewing small sample by ultrasound [5]. Ultrasound of the facial muscles is feasible and shows moderate to excellent reproducibility [6]. However, there was limited studies that have observed skin thickness, facial arteries and facial muscles together. ultrasound imaging can be used to detect low levels of muscle activity, ultrasound imaging thus providing a non-invasive method of detecting isometric muscle contractions of certain individual muscles [7]. Non-invasive treatment can cause complications from injection points and the materials used in treatment. Filler materials are recognized on ultrasound device, necrosis of fatty tissue and epidermal cysts; the associated dermatopathy was transient, resolving upon disappearance of the filler materials [8]. Ultrasound examination gave an uncomplicated and a reproducible access to parameters of jaw muscle function and its interaction [9]. Ultrasound devices can be used directly by clinician and the medical staff. clinical diagnosis and treatment in efficient manner prior to treatment of patient could be possible. After the sonography inspection, a process leading directly to the treatment step is possible. Ultrasound examination used in the head and neck oncology, with fine needle aspiration biopsy is an accurate method for the assessment [10].
Thus, we provide measured data of arterial in depth to be applicable in the non-invasive procedures and fields of dentistry. However, ultrasound diagnosis can be combined with various procedures and operations while aiding selection of lymph nodes suitable for incisional biopsy prior to surgery and positioning of the surgery for better and safer treatment [4]. By understanding the relationship and characteristics of the anatomical structure based on the existing anatomical landmarks of the face, we measure the distance from the surface to skin thickness, fat, surrounding muscles, and suggest the basic depth of the facial artery. In addition, we observed how the ultrasound diagnosis device depicted detailed face artery and surrounding structures to evaluate its feasibility in clinical implications. In this research, we stabilized the measurement by removing any type of shakings to minimize the error range and distinguish bloodstream according to the intensity of the signal by the power doppler function.
Therefore, the aim of this study is to provide useful information regarding precise depth of the facial artery and its surrounding tissues.
In this research, a total of 40 Korean volunteer participants (23 males and 17 females) were used. The requirements of participants were those who did not undergo surgery on the entire face and those who did not receive cosmetic surgery on the face within the recent 6 months. Research participants included vulnerable subjects, and experiments were conducted after obtaining test participation consents from volunteers in advance. This research plan was carried out after IRB approval by the Institutional Bioethics Committee (IRB No. 2-2017-0023).
The ‘Ultrasound diagnosis device’ transducer is divided into two major types. Spherical transducers are used for large organ examination at depths with 3-5 MHz frequency. A 5-15MHz frequency linear transducer is used for shallow structure observation. A low frequency is appropriate for observing deep structures. A high frequency increases the resolution, while the penetration depth is limited to a shallow depth. A low frequency decreases the resolution, while the penetration depth is extended to deep depth [4]. In this research, a linear transducer, a hockey stick shape, with a frequency of 15MHz (B-mode) was used to observe the detailed structure of the face.
Doppler function of ultrasound devices has color doppler and power doppler pulse and is useful to observe the blood vessel condition. Doppler effect refers to a phenomenon in which the frequency of a sound wave reflected from a moving tissue is changed when a sound wave originating from a transducer returns from approaching red blood cell, the increased frequency indicates that bloodstream is coming toward the transducer, is recognized as positive, and is depicted as color red-yellow <Fig. 1>. When the reflected frequency from departing red blood cell comes in, the bloodstream is recognized as negative and is depicted as color blue <Fig. 2>.
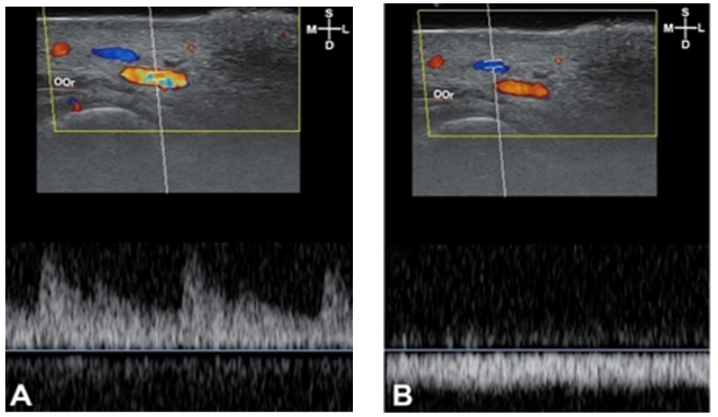
Fig. 1. Bloodstream sonography of F4: pumping bloodstream image (A) indicates arterial flow. Flowing bloodstream image (B) indicates the venous flow. S: superficial; D: deep; M: medial; L: lateral
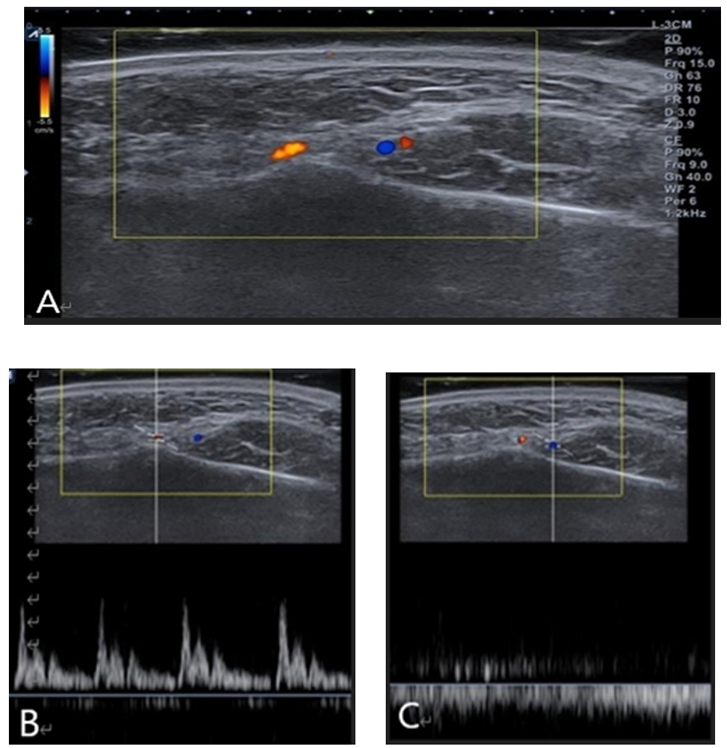
Fig. 2. Doppler image color indication (A), and doppler power pulse image; pumping flow indicates the artery (B), and doppler power pulse image; flowing image indicates the vein (C). Yellow: artery, blue: vein
Doppler provides information about bloodstream, but there is a disadvantage that patient movement and transducer shaking can also be misdiagnosed as bloodstream.
Based on the previously published anatomical reference points, total 5 points of F1, F2, F3, F4, and F5 were pre-decided; F1: antegonial notch, F2: midway point between F1 and F3, F3: 1 cm away from cheilion, F4: the midway point between F3 and F5, and F5: nasal alare <Fig. 3>.
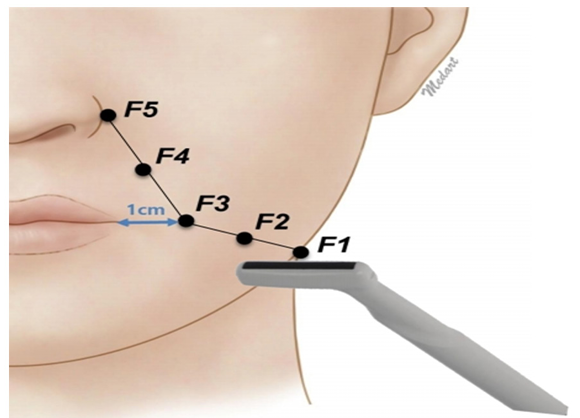
Fig. 3. Facial landmarks: F1: antegonial notch; F2: midpoint between F1 and F3; F3: 1 cm lateral to cheilion; F4: midpoint between F3 and F5; F5: nasal alare
E-Cube 15 EX (Alpinion Seoul, Korea) was used to film the sonography images the left face of over all 40 test volunteers. A I-08-17 hockey stick type transducer capable of precisely photographing the curved part was used to film even measurement of 3 cm deep in the transverse direction. Sono Gel was put on the skin to a thickness of about 2 cm in the diagnosis of ultrasound detection so that the skin was not pressed. The procedure was to place the transducer in a thickened file of gel maintaining a 5 mm clearance from the skin to prevent the transducer from pressing on the skin. First, the lips were protruded and pursed to distinguish facial muscles and structures at each point. The order of filming at each designated mark point are as follows.
(1) The test volunteers moved facial muscles around the lips to distinguish facial muscles from the structure while the sonography and the doppler image P2 (Picture2: movie saving function) were recorded.
(2) Doppler function was turned on to distinguish the artery and vein.
(3) Pulse (artery, vein) image filming.
(4) Doppler image filming.
(5) Sonography image filming.
The data used in the research were obtained from a total of 4 sites images (sonography, doppler, pulse (artery, vein)) and 2 images (sonography, doppler) from one test participant. ImageJ program was used to obtain the thickness of the skin in the sonography image and the distance from skin to dermis: subcutaneous tissue, fat, muscles, facial artery. In addition to those, the distance to the observed face artery was measured in color doppler images <Fig. 4>.
The measurement of the ImageJ proceeded as follows. Since the center of the sonography image is the landmark point marked in advance, the scale distance set by 10 mm, scale wand was used to measure vertically downward from the center skin of the sonography. Facial muscles were measured at the nearest to the facial artery.
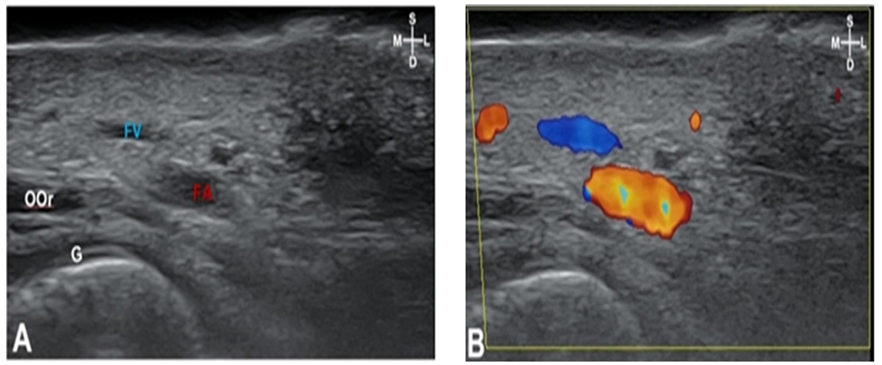
Fig. 4. Measurement of sonography: sonography of F1 (A), sonography of F2 (B), Measuring the skin thickness, fats and depth of facial artery by using the ImageJ program. Yellow bar, scale wand set by 10 mm. DAO: depressor anguli oris; Mn: mandible; S: superficial; D: deep; M: medial; L: lateral
The facial artery was observed at 5 points of 40 subjects, and there were no cases showing pathologic anatomical variations when the surrounding structures were observed.
The average depth and standard deviation from the skin to the facial artery was 9.3±2.2 mm in F1 (antegonial notch), 8.8±3.0 mm in F2 (a midpoint between F1and F3), 6.9±3.5 mm in F3 (1 cm lateral to cheilion), 4.8±1.4 mm in F4 (a midpoint between F3 and F5), and 5.0±1.6 mm in F5 (nasal alare). The thickness of the skin was the thinnest at 1.6 mm in F4 and the thickest at 2.3 mm in F5. The facial artery was located deepest with a depth of 9.3 mm in F1 while shallowest with a depth of 4.9 mm in F4 <Table 1>.
In F1, the facial artery was observed located along the medial margin of the masseter muscle <Fig. 5>. The peripheral structures observed in F2, F3, and F4 were facial muscles, while depressor anguli oris muscles was observed in F2, and orbicularis oris muscles were observed in F3 and F4, respectived <Fig. 6>.
Table 1. Thickness of skin and depth measurement from skin to the facial artery of each landmark (F1-F5) [(Unit: mean±SD, mm)]
| Land mark | Skin thickness | Arterial depth |
|---|---|---|
| F1 | 2.0±0.6 | 9.3±2.2 |
| F2 | 2.2±0.5 | 8.9±3.0 |
| F3 | 1.9±0.6 | 6.9±3.5 |
| F4 | 1.6±0.5 | 4.9±1.4 |
| F5 | 2.3±1.0 | 5.0±1.6 |
SD: standard deviation
Depressor anguli oris muscles were observed in F2, and the depth from skin to depressor anguli oris muscles was 8.6±2.1 mm, and this muscle was observed in 90% of 40 cases. Orbicularis oris muscles were observed in F3 and F4 <Fig. 5,6>. The depth from skin to orbicularis oris muscles was 9.5±3.3 mm in F3 and 6.3±3.1 mm in F4, respectively <Table 2>.
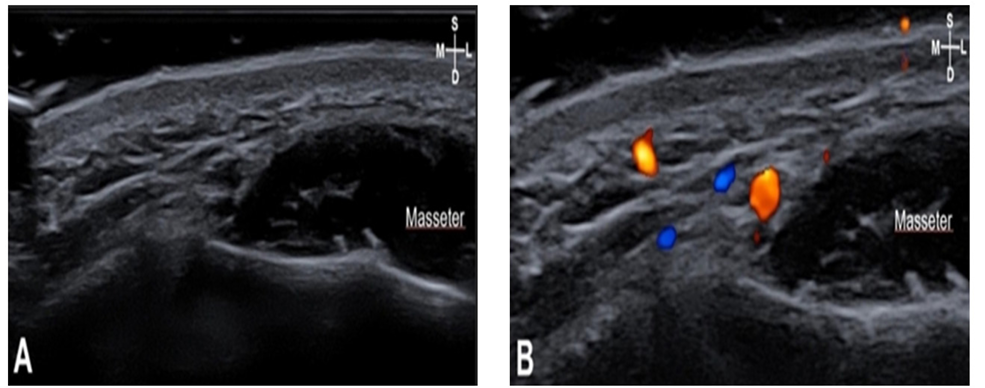
Fig. 5. Sonography (A) and doppler image (B) of F3: The arteries were located posterior to the orbicularis oris (OOr). The depth of the facial artery is 6.9 mm. Depth of skin to the OOr is 9.5mm. The dotted line, OOr located in arch shape; Blue, facial artery; S: superficial; D: deep; M: medial; L: lateral
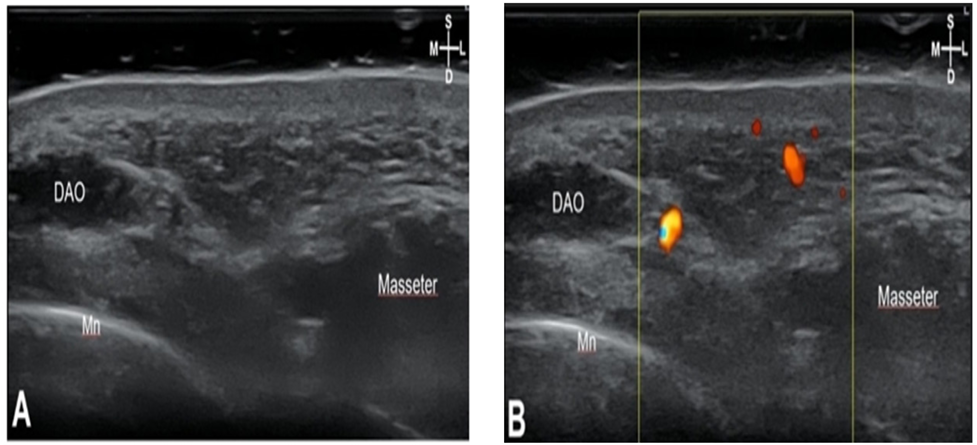
Fig. 6. Sonography (A) and doppler image (B) of F4: Arterial depth of F4 is 4.9mm, skin to the orbicularis oris (OOr) depth is 6.3 mm. S: superficial; D: deep; M: medial; L: lateral; Yellow: facial artery; Blue: facial vein
Table 2. Depth measurement and detection rate from skin to depressor anguli oris and skin to orbicularis oris [(Unit: mean±SD, mm)]
| Muscle | Landmark | Depth | Detection Rate (%) |
|---|---|---|---|
| DAO | F2 | 8.6±2.1 | 90.0 |
| OOr | F3 | 9.5±3.3 | 77.5 |
| F4 | 6.3±3.1 | 62.5 |
DAO: depressor anguli oris; OOr: orbicularis oris
In F5, it was confirmed that the facial artery was located right next to the nasal alare from F1 to F5, the thickness of the skin was similar, but it became slightly thicker toward F5, and it was observed that the facial artery was located gradually closer to the skin from F1 to F5 as it was facing the surface of the skin <Fig. 7>.
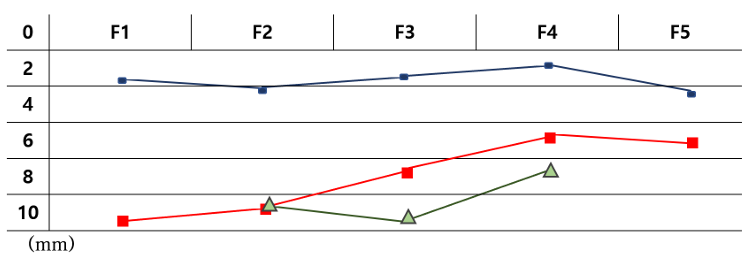
Fig. 7. Skin thickness (blue), arterial depth (red) and muscle depth of the depressor anguli oris (F2) and the orbicularis oris (F3, F4) (green): Observed muscles was located closer to the facial artery from F2-F3 F4. The thickness of the skin were similar toward the center of the face though it became slightly thicker. The facial artery becomes shallow, toward the surface when it gets closer to the center of a face from F1 to F5.
The blood supply to the face is made by the complex distribution of multiple arteries [11]. all among these, the facial artery is the largest artery and plays a vital role in the blood supply to the face area.
As the facial skin sags with age, such as the jaw-line wrinkles around the mouth, the mouth is aesthetically at a disadvantage. A lot of cosmetic procedures such as filler injection are performed at this area. It is imperative that the clinical doctors know the depth of the facial artery because cosmetic surgery can cause fatal side effects when Botulinum toxin injection or filler material is mistakenly injected. Therefore, it requires sufficient anatomical knowledge in non-invasive diagnosis and minimal-invasive surgery. Recently, side effects such as parenchyma necrosis and skin discoloration due to vascular damages have been frequently reported in injecting fillers. Previous studies reported that 21.4% of the filler side effects was parenchyma necrosis and skin discoloration [12]. Besides these side effects, non-invasive procedures can cause fatal side effects such as skin necrosis and blindness. Therefore, anatomical data about the depth of facial arteries are essential to avoid arteries during non-invasive treatments or minimal-invasive surgery. There are studies on the course and distribution of the facial arteries, but there is no study on their depth. In this study, the depth of facial artery, including muscle, was observed through an ultrasound device.
In F2, depressor anguli oris muscles were observed, and the depth was 8.6±2.1 mm. The depth of the facial artery at F2 was 8.9±3.0 mm. The orbicularis oris muscles were observed at F3 and F4. At F3, the depth of orbicularis oris muscles was 9.5±3.3 mm, and the depth of a facial artery was 6.9±3.5 mm. At F4, the depth of orbicularis oris muscles was 6.3±3.1 mm, and the depth of the facial artery was 4.9±1.4 mm. In this study, the facial muscles were located deeper than the facial arteries in terms of mean values. However, the relationship between these facial muscles and arteries may vary depending on the person.
The facial artery was observed in the deep layer of the facial muscles, and the depth of the facial artery at the nasolabial fold was 5 mm. [13]. The nasolabial fold point corresponds to F4 of this study and F4’s facial artery measurement value was 4.9±1.4mm. The measurement value of the facial artery is vital for the prevention of side effects such as skin necrosis and various complications due to ischemia phenomenon caused by pressure to blood vessels or extra-vascular during various treatments such as minimal-invasive procedures and other non-invasive procedures. As we have seen, the facial artery was found to be closer to the skin, rising from F1 to F5 toward the surface. F3 and F4, which were getting closer to the skin, are located near the winding portion where the facial artery is directed meanderingly toward the surface, and there is no muscle covering the facial artery.
Therefore, nasolabial fold wrinkle relief filler injection in this area could be accompanied by bruising or edema when the facial artery is damaged during the procedure, the entry point of the cannula is 1-5 mm inward from the nasolabial fold. The injection is performed retro-grade above the orbicularis oris muscles [14]. The depth of the orbicularis oris muscles was 9.5±3.3 mm, and the depth of the facial artery was 6.9±3.5 mm, which were located shallower than the orbicularis oris muscles at F3 of this study. Because the facial artery is located shallower than the orbicularis oris muscles, the cannula or needle can easily injure the facial artery and result in bruise and hematoma.
Based on the results of the study, it would be safe to adjust the insertion depth of the cannula to 3 mm or less to reduce side effects such as skin discoloration, blindness, and skin necrosis. Besides, it is advised to avoid the use of a cannula with a diameter of 27 G or more to prevent penetration or tearing of blood vessels. However, since the use of a cannula cannot guarantee the non-occurrence of vascular injury, it should be injected slowly to check hematoma during the procedures. When proceeding non-invasive procedures, to improve the marionette line, care should be taken not to inject filler around the F1. Especially at F1, the depth of the facial artery was observed as 9.3±2.2 mm, thus needs to avoid stinging needle not deeper than 7 mm deep.
In this study, results come with statistically averaged data, though depending on the person the location of the facial artery is possibly located anterior or posterior to the muscle for each landmark. In addition to the study on the course direction of the facial artery of previous study, we focused on an anatomical study data on living subjects, by ultrasound devices. The preview studies do not have much data to suggest the depth from the skin to the facial artery. To overcome the limitation that the cadaver is dried or the muscles blood vessels are pressed in the process of dissection, this study on ultrasound diagnosis was performed to detect anatomical structures of living subjects. It was possible to observe the undamaged facial artery and surrounding anatomical structures.
This study provides the in depth value of the facial artery and anatomic structure to the clinic doctors and the researchers and could be used as the guideline for the non- invasive surgery or minimal invasive procedures in medical and dentistry fields. This study provided basic data of the anatomical research of cosmetic surgery and non-invasive surgeries, for the other anatomical related studies and future research.
This study confirmed that an anatomical structure of a living person could be identified using an ultrasound device. The first non-invasive anatomic study was created by using ultrasound devices that were only used for diagnosis or examination.
1. This study is based on the 40 samples could actually measure the structure of a living person, and no other personal information was referenced. Facial shape, gender, age, and BMI were not referenced. The facial artery was observed at 5 points of 40 subjects, and there were no cases showing pathologic anatomical variations when the surrounding structures were observed.
2. The measurement of the structure with the aid of ImageJ computer program can also be seen to have measured the depth within the minimized error range. The average depth and standard deviation from the skin to the facial artery was 9.3±2.2 mm in F1 (antegonial notch), 8.8±3.0 mm in F2 (a midpoint between F1and F3), 6.9±3.5 mm in F3 (1 cm lateral to cheilion), 4.8±1.4 mm in F4 (a midpoint between F3 and F5), and 5.0±1.6 mm in F5 (nasal alare). The thickness of the skin was the thinnest at 1.6 mm in F4 and the thickest at 2.3 mm in F5.
The results of this study provide useful information regarding precise depth of the facial artery for clinical application in the dentistry fields and non-invasive surgery. Research using medical instruments will continue with existing anatomical studies and will show infinite varieties in anatomical researches. Enhancement in these studies will provide more data for the medical community in the future. If there is an ultrasonic device in the local clinic, it may be a reasonable method to examine the structure before the procedure. and a comprehensive study will be conducted by referring to it in future studies.
Conceptualization: YN Han, KS Hu; Data collection: YN Han; Formal analysis: YN Han; Writing-original draft: YN Han; Writing review& editing: YN Han, KS Hu
The authors declared no conflicts of interest.
None.
This study was approved by the Institutional Review Board (IRB) of Yonsei University (IRB No. 2-2017-0023).
Data can be obtained from the corresponding author.
None.
Yang HM, Lee YI, Lee JG, Choi YJ, Lee HJ, Lee SH, et al. Topography of superficial arteries on the face. Anat Biol Anthropol 2013;26(4):131-40. https://doi.org/10.11637/kjpa.2013.26.4.131.
Koh KS, Kim HJ, Oh CS, Chung IH. Branching patterns and symmetry of the course of the facial artery in Koreans. Int J Oral Maxillofacial Surg 2003;32(4):414-8. https://doi.org/10.1054/ijom.2002.0372.
Yang HM, Lee JG, Hu KS, Gil YC, Choi YJ, Lee HK, et al. New anatomical insights on the course and branching patterns of the facial artery: clinical implications of injectable treatments to the nasolabial fold and Naso jugal groove. Plast Reconstr Surg 2014;133(5):1077-82. https://doi.org/10.1097/PRS.0000000000000099.
Kim JK. Ultrasound of head and neck: anatomy. Korean J Otorhinolaryngology-Head Neck Surg 2016;59(4):265-72. https://doi.org/10.3342/kjorl-hns.2016.59.4.265.
Benington PC, Gardener JE, Hunt NP. Masseter muscle volume measured using ultrasonography and its relationship with facial morphology. Eur J Orthod 1999;21(6):659-70. https://doi.org/10.1093/ejo/21.6.659.
van Alfen N, Gilhuis HJ, Keijzers JP, Pillen S, van Dijk JP. Quantitative facial muscle ultrasound: feasibility and reproducibility. Muscle Nerve 2013;48(3):375-80. https://doi.org/10.1002/mus.23769.
Hodges PW, Pengel LHM, Herbert RD. Gandevia SC. Measurement of muscle contraction with ultrasound imaging. Muscle Nerve 2003;27(6):682-92. https://doi.org/10.1002/mus.10375.
Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GBE. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Veneteol 2012;26(3):292-301. https://doi.org/10.1111/j.1468-3083.2011.04047.x.
Bakke M, Tuxen A, Vilmann P, Jensen BR, Vilmann A, Toft M. Ultrasound image of human masseter muscle related to bite force, electromyography, facial morphology, and occlusal factors. Scand J Dent Res 1992;100(3):164-71. http://doi.org/10.1111/j.16000722.tb01734.x.
de Jong RJB, Rongen RJ, Lameris JS, Harthoorn M, Verwoerd CD, Knegt P. Metastatic neck disease. Palpation vs ultrasound examination. Arch Otolaryngol Head Neck Surg 1989;115(6):689-90. https://doi.org/10.1001/archotol.1989.01860300043013.
Yu SK, Lee KY, Lee MH, Jeon HY, Kang H, Lee CK, Kim HJ. Morphometric analysis of the facial artery in perioral region. Korean J Phys Anthropol 2014;27(4):179-86. https://doi.org/10.11637/kjpa.2014.27.4.179.
Park TH, Seo SW, Kim JK, Chang CH. Clinical experience with hyaluronic acid-filler complications. J Plast Reconstr Aesthet Surg 2011;64(7):892-6. https://doi.org/10.1016/j.bjps.2011.01.008.
Lee JG, Yang HM, Choi YJ, Favero V, Kim YS, Hu KS, et al. Facial arterial depth and relationship with the facial musculature layer. Plast Reconstr Surg 2015;135(2):437-44. https://doi.org/10.1097/PRS.0000000000000991.
Kim HJ, Seo KK, Lee HK, Kim JS. Clinical anatomy for botulinum toxin injection. In Kim HJ, Youn KH, Kim JS, Hong SO, Na J: Edited Clinical anatomy of the face for filler and botulinum toxin injection. 1st ed. Singapore: Springer; 2016: 55-92. https://doi.org/10.1007/978-981-10-0240-3.