
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Yae-Hoon Kim1![]() , Gyu-Bin Kim1
, Gyu-Bin Kim1![]() , Seung-Yeon Wi1
, Seung-Yeon Wi1![]() , Khadija-Ashraf2
, Khadija-Ashraf2![]() , Kang-Jae Lee2
, Kang-Jae Lee2![]() , Dong Liu3
, Dong Liu3![]() , Yun-Sook Jung1,4
, Yun-Sook Jung1,4![]()
1Department of Dental Hygiene, Graduate School of Kyungpook National University
2Department of Convergence and Fusion System Engineering, Kyungpook National University
3School of Humanities and Social Science, The Chinese University of Hong Kong, Shenzhen
4Department of Dental Hygiene, College of Science & Technology, Kyungpook National University
Correspondence to Yun-Sook Jung, Department of Dental Hygiene, College of Science & Technology, Kyungpook National University 2559 Gyeongsang-daero, Sangju-si, Gyeongsangbuk-do, 37224, Korea. Tel: +82-54-530-1425, E-mail: ysjung0313@knu.ac.kr
Volume 25, Number 6, Pages 545-53, December 2025.
J Korean Soc Dent Hyg 2025;25(6):545-53. https://doi.org/10.13065/jksdh.2025.25.6.8
Received on November 14, 2025, Revised on December 02, 2025, Accepted on December 05, 2025, Published on December 30, 2025.
Copyright © 2025 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: This study aimed to examine the association between regional accessibility to dental services and the utilization of preventive dental care in Korea. Methods: We combined data from the 2024 Korean Community Health Survey with data from public databases, including KOSTAT and Health Insurance and Review Assessment (HIRA). The final analysis included 231,554 participants. Preventive dental-care utilization was defined as having undergone dental scaling within the previous year. Access to dental services was calculated as the number of dental-care personnel per 10,000 people in the 252 administrative districts. After adjusting for age and education level, we performed a composite sample logistic regression analysis using SAS 9.4. The spatial distribution was visualized using QGIS 3.40.11. Results: Among participants, 50.6% reported having undergone dental scaling in the past year. In the adjusted model, individuals residing in areas with high accessibility to dental services had significantly higher odds of receiving annual scaling (odds ratio=1.310; confidence interval: 1.27–1.35) compared with those residing in areas with low accessibility (p<0.001). Conclusions: Greater access to dental services was associated with a higher likelihood of utilizing preventive dental care. Strengthening local dental infrastructure is essential for reducing the regional oral health gap.
Community health services, Dental clinics, Dental scaling, Oral health, Public health infrastructure
Health is a fundamental human right, influenced not only by individual lifestyle habits but also by social, economic, and environmental conditions. In particular, accessibility to healthcare service is main determinant of the population’s health status, and unequal distribution of medical institutions and resources has been identified as a major factor that exacerbates regional health disparities [1]. Residents in areas with high accessibility to healthcare service can more easily obtain early diagnosis and preventive care, thereby maintaining better health, whereas those living in areas with low accessibility tend to show higher prevalence of chronic disease and premature mortality due to limited healthcare utilization [2,3]. Healthcare accessibility encompasses more than geographic distance, it is also shaped by spatial and structural factors such as the number and density of healthcare facilities, transportation networks, and the overall distribution of medical resources [4]. Such accessibility issues are equally evident in the field of oral health. Although most oral diseases are preventable, areas with limited access to dental care tend to have fewer opportunities for regular check ups and preventive treatments, thereby leading to oral health inequalities [5]. Oral health is regarded as a component of overall health, directly linked to systemic health, nutritional status, social relationships, and mental state [6]. Prevention of oral disease can be achieved not only through individual oral hygiene management, but also through community based preventive care and effectiveness. Since July 2013, Korea has implemented a policy to cover scaling for adults aged 20 years or older through health insurance, aiming to expand preventive oral health services. This policy is evaluated as a representative public health policy that has contributed to raising public awareness of oral health and expanding opportunities for preventive dental care. According to the ‘Analysis of Dental Outpatient Treatment Status’ by the Health Insurance Review & Assessment Service, the scaling examination rate has steadily increased from approximately 24.7% in 2018 to 29.7% in 2022 since scaling was covered by insurance, and prevention oriented oral health behaviors have shown a gradual spread. Dental scaling, by removing dental biofilm, calculus, and food debris, alleviates inflammation of the periodontal tissues and helps prevent the recurrence of periodontal disease. It has also been reported to be associated with reductions in systemic inflammatory responses and the prevention of metabolic disorders [7]. Furthermore, factors reported to influence the experience of dental scaling have typically included individual and psychosocial characteristics such as sex, age, educational attainment, income level, smoking, stress, and self-rated oral health [8]. In addition, National Health Insurance eligibility type and area-level characteristics have been identified as important determinants, with evidence showing higher preventive dental care utilization among groups with higher income and education [9]. However, previous studies have primarily focused on individual-level factors such as age and income. In contrast, relatively few studies have examined how structural accessibility such as the spatial distribution of dental resources or the density of dental clinics affects utilization and quality of care. Although a recent study by Lee [10] reported regional disparities between the distribution of dental resources and utilization patterns, such research remains limited. Also In the field of public health, GIS has been widely used to identify medically underserved areas and to analyze accessibility to healthcare facilities [11]. However, QGIS based spatial analyzes focusing on the distribution of dental care resources or the utilization of dental scaling services remain considerably limited.
Therefore, this study aimed to analyze the relationship between accessibility to dental services and preventive dental care use among community residents. Using data from the Korea Community Health Survey (KCHS), conducted annually by the Korea Disease Control and Prevention Agency, we examined the association between regional dental clinic density (an indicator of accessibility) and the rate of dental scaling among adults. In particular, as the 2024 KCHS reintroduced questions related to scaling, it enabled a recent comparison and analysis of regional differences in preventive oral health behaviors. This study aims to identify the impact of regional dental service accessibility on preventive dental utilization, thereby providing basic data for alleviating regional oral health inequalities and establishing prevention focused oral health policies.
This study utilized raw data from the 2024 Korea Community Health Survey. The Community Health Survey is an annual, on-site interview survey conducted on households nationwide, targeting adults aged 19 and older, and is a nationally approved statistical data (Approval number 117075). A total of 231,554 individuals who provided responses regarding sex, education level, and annual scaling experience were included in the analysis, while 175 respondents who did not answer the scaling experience were excluded. The Community Health Survey is not classified as human-subject research under Article 2, Paragraph 2 of the Enforcement Regulations of the Bioethics and Safety Act, and is therefore exempt from institutional review board (IRB) review. This study analyzed the combined effects of individual-level annual scaling experience and regional-level dental clinic distribution to evaluate the impact of local dental service accessibility on preventive dental care utilization.
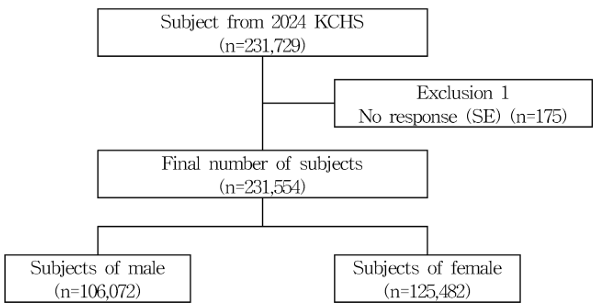
Fig. 1. Flow chart of the study subject
KCHS: Korea Community Health Survey; SE: Annual scaling experience
This study utilized data from the 2024 Korea Community Health Survey (KCHS) by the Korea Disease Control and Prevention Agency (KDCA) to calculate the regional prevalance of annual dental scaling. Additionally, population size and the number of dental clinics by region were derived using data from the 2024 Population and Housing Census by Statistics Korea (KOSTAT) and dental clinic information from the Health Insurance Review and Assessment Service (HIRA).
The dependent variable in this study was the utilization of preventive dental care, measured by responses to the KCHS question asking “whether individuals had recevied dental scaling within the past year”. Responses were categorized into ‘yes’ and ‘no’ for analysis. Dental scaling is a representative preventive dental care use behavior and an important indicator for preventing oral diseases and maintaining oral hygiene. In this study, it was used as an indicator reflecting the level of experience in using preventive dental care among community residents.
The independent variable was defined as dental service accessibility. Accessibility was calculated as the number of dental clinics per 10,000 population, derived by standardizing the number of dental clinics in each of the 252 administrative districts based on the population size of each district.

The continuous indicator was categorized into three groups ‘high,’ ‘medium,’ and ‘low’ based on tertiles to enhance clarity in regional comparisons. This indicator reflects the density of dental clinic infrastructure relative to the population within each region.
To account for individual level confounding factors that may influence the relationship between regional dental service accessibility and annual scaling experience, age (19-44, 45-64, 65-74, and ≥75 years) and education level (elementary school or lower, middle school, high school, college, and graduate or higher) were included as covariates in the analysis.
Data were analyzed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Since the 2024 Korea Community Health Survey (KCHS) is based on a complex sampling design with stratification, clustering, and weighting, sampling weights were applied to ensure the accuracy of statistical estimates. The general characteristics of the study participants were presented as weighted frequencies and percentages. Differences in annual scaling experience according to sociodemographic characteristics were analyzed using a complex-sample cross-tabulation, and statistical significance was assessed using the Rao–Scott χ² test. The association between access to dental services and annual scaling experience was examined using complex-sample logistic regression analysis. Model 1 presented Unadjusted estimates including only independent variables, while Model 2 was adjusted for age and education level. Results were expressed as odds ratios (OR) with 95% confidence intervals (CI), and statistical significance was set at p<0.05.
The geographic distribution of dental service accessibility by region (city, county, and district) was visualized using Quantum Geographic Information System (QGIS), version 3.40.11 (QGIS Development Team, 2025) in the form of a choropleth map. Administrative boundary data for cities, counties, and districts were obtained from the Ministry of Land, Infrastructure and Transport of Korea, and the dental service accessibility index was mapped at the city/county/district level.
A total of 231,554 participants were included in the study, comprising 106,072 men (49.5%) and 125,482 women (50.5%). By age group, 61,243 participants (39.0%) were aged 19–44 years, 86,624 (37.7%) were aged 45–64 years, 45,630 (13.6%) were aged 65–74 years, and 38,057 (9.7%) were aged 75 years or older, with the 19–44-year group being the largest. Regarding educational level, 16,739 participants (3.2%) had an education level of elementary school or below, 31,444 (7.7%) had middle school, 25,056 (7.7%) had high school, 75,943 (34.8%) had some college, and 82,372 (46.5%) had a college degree or higher, indicating a relatively high proportion of highly educated individuals. In terms of dental service accessibility, 18.6% of participants lived in areas with low accessibility, 30.9% in moderate-accessibility areas, and 50.5% in high-accessibility areas <Table 1>.
Table 1. General characteristics of the study population Characteristics [Unit: N(%)]
| Characteristics | Total |
|---|---|
| Total | 231,554(100.0) |
| Gender | |
| Male | 106,072(49.5) |
| Female | 125,482(50.5) |
| Age (yr) | |
| 19-44 | 61,243(39.0) |
| 45-64 | 86,624(37.7) |
| 65-74 | 45,630(13.6) |
| 75≤ | 38,057(9.7) |
| Education | |
| ≤Elementary school | 16,739(3.2) |
| Middle school | 31,444(7.7) |
| High school | 25,056(7.7) |
| College | 75,943(34.8) |
| Graduated | 82,372(46.5) |
| Dental service accessibility* | |
| High | 77,577(50.5) |
| Middle | 75,724(30.9) |
| Low | 78,253(18.6) |
*included dental hospital and clinic
Among all participants, 117,196 (50.6%) reported having undergone scaling within the past year. By gender, women (64,480; 51.4%) had a higher prevalence of annual scaling experience than men (52,716; 49.7%) (p<0.001). By age group, the prevalence was relatively higher among those aged 45–64 years (49,554; 57.2%) and 19–44 years (34,656; 56.6%), but sharply decreased among those aged 75 years or older (9,719; 25.5%) (p<0.001). A significant positive association was observed between educational level and annual scaling experience. Participants with elementary school education or below (3,055; 18.3%) had the lowest prevalence, whereas those with a college degree or higher (51,358; 62.9%) showed a substantially higher rate (p<0.001). In terms of dental service accessibility, participants living in high-accessibility areas (44,620; 57.5%) had a significantly higher prevalence of annual scaling experience compared to those in moderate-accessibility (37,923; 50.1%) and low-accessibility areas (34,653; 44.3%) (p<0.001) <Table 2>.
Table 2. Distribution of scaling experience by sociodemographic characteristics in Korea [Unit: N(weighted %)]
| Characteristics | Total | SE** | p* | |
|---|---|---|---|---|
| Yes | No | |||
| Total | 231,554(100.0) | 117,196(50.6) | 114,358(49.4) | |
| Gender | ||||
| Male | 106,072(49.5) | 52,716(49.7) | 53,356(50.3) | <0.001 |
| Female | 125,482(50.5) | 64,480(51.4) | 61,002(48.6) | |
| Age (yr) | ||||
| 19-44 | 61,243(39.0) | 34,656(56.6) | 26,587(43.4) | <0.001 |
| 45-64 | 86,624(37.7) | 49,554(57.2) | 37,070(42.8) | |
| 65-74 | 45,630(13.6) | 23,267(51.0) | 22,363(49.0) | |
| 75≤ | 38,057(9.7) | 9,719(25.5) | 28,338(74.5) | |
| Education | ||||
| ≤Elementary school | 16,739(3.2) | 3,055(18.3) | 13,684(81.7) | <0.001 |
| Middle school | 31,444(7.7) | 10,901(34.7) | 20,543(65.3) | |
| High school | 25,056(7.7) | 11,636(46.4) | 13,420(53.6) | |
| College | 75,943(34.8) | 40,246(53.0) | 35,697(47.0) | |
| Graduated | 82,372(46.5) | 51,358(62.3) | 31,014(37.7) | |
| Dental service accessibility*** | ||||
| High | 77,577(50.5) | 44,620(57.5) | 32,957(42.5) | <0.001 |
| Middle | 75,724(30.9) | 37,923(50.1) | 37,801(49.9) | |
| Low | 78,253(18.6) | 34,653(44.3) | 43,600(55.7) | |
*by complex sample chi square test; **Annual scaling experience; ***included dental hospital and clinic
In the unadjusted model, the odds ratio (OR) for areas with high accessibility was 1.417 (95% CI: 1.38–1.46), and for areas with moderate accessibility, 1.316 (95% CI: 1.10–1.17), both significantly higher than those for low-accessibility areas (p<0.001) <Table 3>. After adjusting for age and educational level, the odds ratios remained consistent: the ‘high’ accessibility group had an OR of 1.310 (95% CI: 1.27–1.35), and the ‘middle’ group had an OR of 1.094 (95% CI: 1.06–1.13), indicating that higher accessibility was consistently associated with a greater likelihood of annual scaling experience (p<0.001) <Table 3>.
Based on the distribution of dental service accessibility and scaling experience rates by region, regions with both ‘high’ dental service accessibility and ‘high’ scaling experience rates included Gangnam-gu in Seoul, Dongnae-gu in Busan, and Gyeyang-gu in Incheon. Regions with ‘middle’ dental service accessibility and ‘middle’ scaling experience rates included Wonju-si in Gangwon state, Yeoncheon-gun in Gyeonggi-do, and Gunsan-si in Jeonbuk state. Regions with ‘low’ dental service accessibility and ‘low’ scaling experience rates included Namhae-gun in Gyeongsangnam-do, Gurye-gun in Jeollanam-do, and Bonghwa-gun in Gyeongsangbuk-do. Overall, the regional distribution of scaling experience rates showed a pattern consistent with level of dental service accessibility <Fig. 2,3.>.
Table 3. Logistic regression analysis of association between dental service accessibility and experience of scaling
| Factors | Model 1 | Model 2 | ||
|---|---|---|---|---|
| OR*(95% CI)* | p** | OR*(95% CI)* | p** | |
| Dental service accessibility | ||||
| Low | 1.000 | 1.000 | ||
| Middle | 1.316(1.10-1.17) | <0.001 | 1.094(1.06-1.13) | <0.001 |
| High | 1.417(1.38-1.46) | <0.001 | 1.310(1.27-1.35) | <0.001 |
Model 1: Unadjusted model; Model 2: Adjusted by age, education
OR: odds ratio; CI: confidence interval
*OR and 95% CI were derived from complex-sample logistic regression models.
**by logistic regression analysis
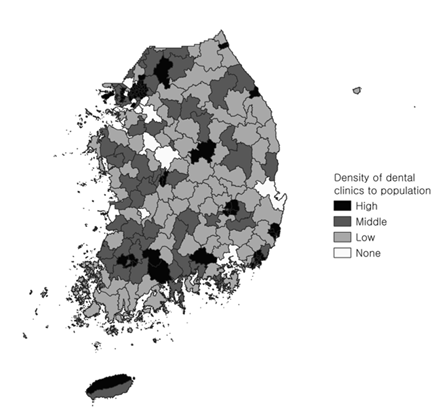
Fig. 2. Regional distribution of dental clinic density relative to population in Korea
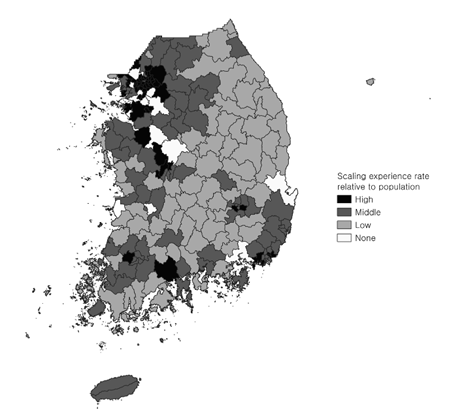
Fig. 3. Regional distribution of scaling experience rates relative to population in Korea
Scaling, one of the professional oral care procedures, is a representative preventive dental service that removes calculus and plaque from the tooth surface and periodontal area, playing an important role in preventing oral diseases and maintaining oral hygiene. Despite its preventive benefits, the degree of scaling experience varies according to demographic and socioeconomic characteristics of the population [12]. Therefore, this study analyzed the influence of regional dental service accessibility on the utilization of preventive dental care, focusing on annual scaling experience as representative oral health behavior. Through this, regional inequalities in oral health care were identified.
Data from the Korea Community Health Survey (KDCA), Korea Population and Housing Census (KOSTAT), and the dental clinic and hospital address report (HIRA) were integrated to estimate accessibility at the level of 252 administrative districts (cities, counties, and districts). The results showed that ‘high’ educational attainment was significantly associated with an increased prevalence of annual scaling experience, and that individuals residing in regions with ‘high’ dental service accessibility had significantly higher scaling experience rates (p<0.001). In particular, participants in ‘high’ accessibility regions were approximately 1.3 times more likely to have undergone scaling compared to those in ‘low’ accessibility regions (p<0.001). This relationship remained statistically consistent even after adjusting for major sociodemographic factors such as age, and education level. These findings are consistent with those of Jang et al. [9], who reported that college graduates had significantly higher rates of scaling experience, and with Heidenreich et al. [13], who found that an increase in the number of dentists per child population in the United States was associated with a 1.67% increase in preventive dental service utilization. Such results suggest that geographic disparities in dental care resources directly influence individual preventive oral health behaviors.
The findings of this study highlight the need for region based policies to enhance the physical accessibility of dental care resources in order to achieve equity in oral health. Rural and island areas, where access to dental clinics is limited compared to urban areas, are likely to have lower utilization rates of preventive dental care. Therefore, policy strategies should include expanding the public dental workforce, redistributing healthcare resources across regions, strengthening the role of regional oral health centers, and increasing the provision of mobile dental services. Moreover, beyond simply increasing the number of facilities, it is essential to improve public awareness of preventive dental care, reform insurance systems, and reduce cost barriers to promote dental service use.
As regional differences in dental service accessibility influence the utilization of preventive dental care, they may contribute to disparities in oral disease experience. Strengthening preventive oral health policies can help shift from a treatment-centered dental care model to a community-based, prevention-oriented approach that promotes equity in oral health.
Unlike previous studies limited to the provincial level, this study has the strength of analyzing preventive dental care utilization at a finer administrative scale (si/gun/gu), thereby enabling a more detailed comparison of regional dental service accessibility. However, this study has several limitations. First, it employed a cross-sectional design, casual inferences between dental service accessibility and preventive dental care utilization cannot be estabilished. Second, annual scaling experience was measured through self-reported responses, which may introduce recall bias and lead to over or under estimation of preventive dental service use. In addition, the use of population level clinic counts does not reflect variations in service quality or the distribution of dental specialties across regions. Finally, dental service accessibility was defined as the number of dental clinics per population a component of structural accessibility the availability of dental resources within a region. However, accessibility is a multidimensional construct that encompasses not only resource density but also geographic proximity, Therefore, the simple ratio of clinics to population may not fully reflect individual’s real world ability to reach and utilize dental services. Future research should incorporate geographic information system (GIS)-based spatial accessibility analyzes and perform multilevel modeling to capture more nuanced regional effects. Such follow-up studies are expected to provide empirical evidence to reduce regional disparities in oral health and to support the development of preventive, equity-oriented national oral health policies. Based on these findings, there is a need to strengthen national policies aimed at improving regional accessibility to dental services and to foster an environment that promotes preventive dental utilization through education and awareness.
This study analyzed the impact of regional accessibility to dental services on preventive dental care utilization using data from the Korea Community Health Survey. The main findings are as follows:
1. Among the total of 231,554 participants, 50.6% had received dental scaling within the past year. The annual scaling experience rate was significantly higher among women, adults under 65 years of age, and individuals with higher educational attainment.
2. The likelihood of having experienced scaling increased as dental service accessibility within a region increased. Individuals living in areas with high accessibility were 1.310 times more likely to have received scaling compared to those in low-accessibility areas. Similarly, residents in regions with moderate accessibility were 1.094 times more likely to have undergone scaling than those in low-accessibility regions. These associations remained consistent even after adjusting for other covariates.
Conceptualization: YH Kim; Data collection: GB Kim; SY Wi, Formal analysis: YS jung, YH Kim, Writing-original draft: YH Kim, GB Kim; SY Wi, Visualization: K Ashraf, KJ Lee, Writing-review&editing: YH Kim, GB Kim, SY Wi, K Ashraf, KJ Lee, L Dong, YS Jung
YS Jung is a member of the Editorial Committee of the Journal of the Korean Society of Dental Hygiene, but was not involved in the review process of this manuscript. The authors declare no other conflicts of interest.
This research was supported by the National Research Foundation of Korea’s 「4-Stage Brain Korea (BK) Graduate School Innovation Support Project」
Non-human or animal research
Data can be obtained from the corresponding author upon reasonable request.
None.