
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
So-Hyeon Lee1![]() , Eun-Jae Choi2
, Eun-Jae Choi2![]() , Hyun-Jae Cho2
, Hyun-Jae Cho2![]() , In-Soon Chang3
, In-Soon Chang3![]() , Yun-Sook Jung1,4
, Yun-Sook Jung1,4![]()
1Department of Dental Hygiene, Graduate School of Kyungpook National University
2Department of Preventive Dentistry & Public Oral Health, and Dental Research Institute, Seoul National University School of Dentistry
3Section of Endodontics, Division of Regenerative and Reconstructive Sciences, School of Dentistry, University of California
4Department of Dental Hygiene, College of Science & Technology, Kyungpook National University
Correspondence to In-Soon Chang, Section of Endodontics, Division of Regenerative and Reconstructive Sciences, School of Dentistry, University of California, Los Angeles, 10833 Le Conte Ave., A3-073 CHS Los Angeles, CA, USA. Tel: +1-310-825-4348, E-mail: ichang@dentistry.ucla.edu
Correspondence to Yun-Sook Jung, Department of Dental Hygiene, College of Science & Technology, Kyungpook National University, 2559 Gyeongsang-daero, Sangju-si, Gyeongsangbuk-do, 37224, Korea. Tel: +82-54-530-1425, Fax: +82-54-530-1429, E-mail: ysjung0313@knu.ac.kr
Volume 25, Number 6, Pages 567-77, December 2025.
J Korean Soc Dent Hyg 2025;25(6):567-77. https://doi.org/10.13065/jksdh.2025.25.6.10
Received on November 17, 2025, Revised on December 01, 2025, Accepted on December 07, 2025, Published on December 30, 2025.
Copyright © 2025 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: In this study, we aimed to identify the prevalence of discrepancies between clinically assessed periodontal status and self-perceived oral health among Korean adults aged 35 years and older, and examine sociodemographic and health-related factors associated with such discrepancies. Methods: Data from 10,146 adults who participated in the 7th Korea National Health and Nutrition Examination Survey were analyzed using complex sample chi-square tests and multivariate logistic regression. The agreement and discrepancy between clinical periodontal status and self-rated oral health were evaluated using the corresponding clinical and subjective measures. Results: A total of 59.7% of participants exhibited a discrepancy between their clinical periodontal condition and self-perceived oral health. Multivariate analysis indicated that individuals who had received mental health counseling within the past year had a significantly higher likelihood of exhibiting such discrepancies, with an odds ratio of 1.496 (95% confidence interval: 1.072–1.496), compared with those who had not received counseling. Conclusions: A substantial proportion of Korean adults inaccurately perceived their periodontal health. Targeted dental hygiene interventions are essential, particularly for individuals whose mental health issues may increase the risk of oral health status misperceptions.
Mental health, Oral health, Oral health status, Periodontal disease, Self-rated oral health, Treatment needs
Health status is generally assessed through two approaches: objective assessments, based on clinical indicators, and subjective assessments, which reflect an individual’s self-perception of health, known as self-rated health (SRH) [1]. Clinical assessments are useful for identifying the presence and severity of diseases; however, they often fail to capture psychosocial factors or quality of life dimensions. In contrast, subjective assessments are closely related to life satisfaction, health behaviors, and healthcare utilization, thus providing valuable information for monitoring health inequalities and developing prevention oriented public health strategies [2,3]. Therefore, a comprehensive understanding of health and the establishment of effective management strategies require consideration of both clinical indicators and subjective perceptions.
However, the correspondence between clinical outcomes and subjective perceptions does not always exist within the same individual. This discrepancy, or health perception gap, directly influences disease management and healthcare seeking behavior, potentially reducing the efficiency of health management [4]. For example, individuals who perceive themselves as healthy despite the presence of disease may miss opportunities for early diagnosis or preventive care [5], whereas perceive themselves as having poor health despite being clinically healthy may experience unnecessary medical use and psychological distress [6].
Such discrepancies are also common in oral health [7,8]. Periodontal disease is often referred to as a “silent disease” because it progresses slowly and painlessly, leading many individuals to underestimate its severity [9,10]. This misperception can delay diagnosis, reduce adherence to professional recommendations, and increase the risk of disease progression, eventually leading to severe periodontitis or tooth loss [11]. Accordingly, the mismatch between clinical periodontal status and subjective perception should be recognized as a critical factor influencing preventive care and public health outcomes rather than a mere perceptual error.
Previous studies have reported that various factors affect this mismatch. Sociodemographic characteristics, including sex, age, education, and income, as well as oral health behaviors, such as toothbrushing frequency, dental visits, and unmet dental needs, have been found to influence self-perceived oral health [12–15]. Furthermore, systemic health status (e.g., presence of chronic diseases) and psychological conditions (e.g., stress, fatigue, and mental health counseling) have been identified as important determinants of subjective health perception [16].
Specifically, mental health status is known to exert a powerful influence on subjective health perception. Psychological distresses, such as depression, anxiety, and stress, can induce a distortion in overall health evaluations, often leading to a pessimistic perception that deviates from the actual clinical status [17]. Furthermore, mental health issues have been reported to compromise oral health management behaviors, consequently elevating the risk of periodontal disease [18]. In addition, some research suggests that subjective oral health perception is more strongly correlated with mental health status than with objective clinical conditions [12,19]. In the context where discrepancies in periodontal disease are common, mental health status is highly likely to act as a crucial factor amplifying the mismatch between clinical periodontal status and subjective oral health perception.
The discrepancy between clinical and subjective health assessments has implications not only for individual selfcare but also for the effectiveness of community oral health policies and promotion programs [20]. Despite this significance, few Korean studies have systematically analyzed mismatches focusing on periodontal disease using nationally representative data and complex survey designs. Given the multifactorial nature of periodontal disease shaped by behaviors, systemic health, and psychological factorsunderstanding the patterns and determinants of this mismatch is crucial [9].
Therefore, this study aimed to analyze data from the 7th Korea National Health and Nutrition Examination Survey (KNHANES, 2016–2018) to determine the prevalence of mismatch between clinical periodontal status, assessed using the Community Periodontal Index (CPI), and subjective oral health perception among Korean adults. Additionally, this study sought to identify sociodemographic, systemic health and mental health-related factors influencing this mismatch. The findings are expected to provide fundamental evidence for developing targeted oral health education, periodontal disease prevention, and public health strategies tailored to adults in Korea.
This study used data from the 7th Korea National Health and Nutrition Examination Survey (KNHANES) conducted from 2016 to 2018. Among the 16,489 participants in the overall health survey and oral examination of the 7th KNHANES, 10,146 individuals aged 35 years and older who had complete information on subjective oral health status and the presence of periodontal disease were selected as the study subjects. According to the decision of the Korea Disease Control and Prevention Agency Institutional Review Board (IRB), the first and second years of the 7th KNHANES were exempt from ethical review, while the third year resumed ethical review to account for the collection of human derived materials and the provision of raw data to third parties, and received approval (Approval No. 2018 01 03 PA)
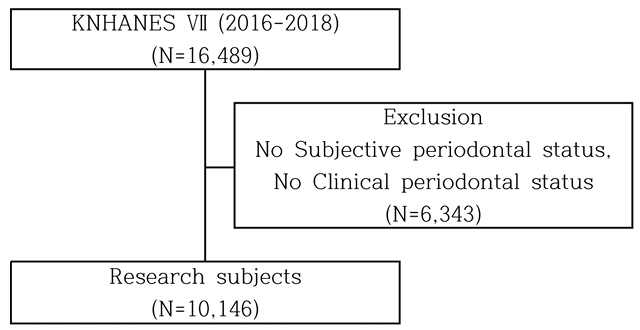
Fig. 1. Research subject selection process
The general characteristics of the study participants included gender, age, education level, income level, smoking status, alcohol consumption, and presence of chronic diseases. Age was categorized into 35–39 years, 40–59 years, and 60 years or older, while education level was classified as middle school or below, high school graduate, and college graduate or higher. Daily toothbrushing frequency related to oral health behavior was categorized as ≤1 time, 2 times, and ≥3 times per day, while unmet dental treatment needs during the past year and oral examination during the past year were dichotomized.
Mental health problems were dichotomized based on whether the participant had received counseling in the past year due to psychological problems, through visits, phone calls, the internet, or other means.
The clinical periodontal status of the study participants was assessed based on the Community Periodontal Index (CPI), as proposed by the World Health Organization (WHO). The CPI divides the mouth into six sections for examination, and the highest score observed is recorded as the representative score. Code 0 indicates a healthy periodontal tissue, Code 1, gingival bleeding; Code 2, calculus formation; Code 3, the presence of shallow periodontal pockets of 4–5 mm; and Code 4, the presence of deep periodontal pockets of 6 mm or more.
Codes 0–2 were classified as having no periodontal disease, whereas Codes 3 and 4 were classified as having periodontal disease.
Subjective oral health status was assessed using a questionnaire in which participants evaluated their perceived oral health. Responses of “very good” and “good” were classified as “good,” while “fair,” “poor,” and “very poor” were classified as “poor,” resulting in two categories for good and poor.
Match and Mismatch were assessed using the previously categorized clinical periodontal status and subjective oral health status variables. If the clinical periodontal status and subjective oral health status response results were identical, they were considered to be a match. On the other hand, cases where the clinical periodontal status and subjective oral health status did not match were considered as Mismatch.
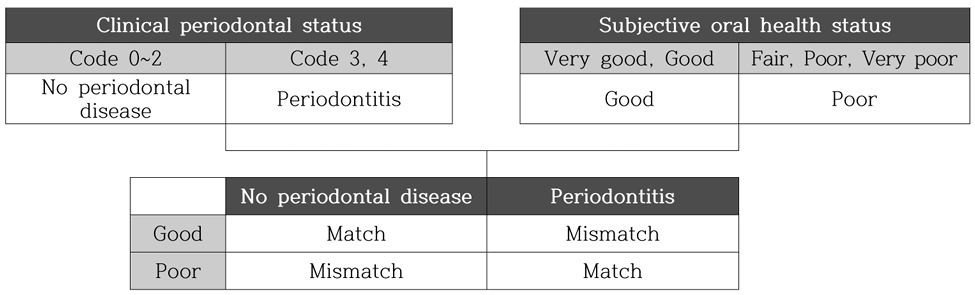
Fig. 2. Classification of match and mismatch between clinical periodontal status and subjective perception
All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA), and the level of statistical significance was set at 0.05. Because the Korea National Health and Nutrition Examination Survey uses a complex sampling design, sampling weights were applied in the analysis. To examine the relationships between Match or Mismatch in clinical periodontal status and subjective perception with general characteristics and health related behaviors, a complex sample chi square test accounting for the complex sampling design was performed.
A total of 10,146 individuals were included in the study, and among them, 59.7% showed mismatch between clinical and subjective oral health status. Analysis of clinical and subjective oral health status according to general characteristics revealed significant differences across all variables, including gender, age, education level, income level, smoking status, and alcohol consumption. The proportion of mismatch was higher in women (65.7%) than in men (51.1%) (p<0.001). The proportion of mismatch by age group was 77.1% among those aged 35–39 years, 61.9% among those aged 40–59 years, and 52.0% among those aged 60 years or older (p<0.001). Mismatch was highest among participants with a college degree or higher (67.9%) (p<0.001), and highest among those in the high income group (62.8%) (p<0.001). In addition, the proportion of mismatch was higher among non-smokers (64.4%) (p<0.001) and higher among non-drinkers (61.2%) (p<0.001) <Table 1>.
Table 1. Match and mismatch between clinical and subjective periodontal status according to general characteristics [Unit: N(%)]
| Characteristics | Total | Clinical and subjective oral health status | p* | |
|---|---|---|---|---|
| Match | Mismatch | |||
| Total | 10,146(100.0) | 4,166(40.3) | 5,980(59.7) | |
| Gender | ||||
| Male | 4,357(41.0) | 2,132(49.7) | 2,225(35.1) | <0.001 |
| Female | 5,789(59.0) | 2,034(50.3) | 3,755(64.9) | |
| Age (yr) | ||||
| 35-39 | 1,218(11.6) | 290(6.6) | 928(15.0) | <0.001 |
| 40-59 | 4,850(48.5) | 1,896(45.9) | 2,954(50.3) | |
| ≥60 | 4,078(39.8) | 1,980(47.5) | 2,098(34.7) | |
| Education | ||||
| ≤Middle school | 3,862(37.7) | 1,881(45.3) | 1,981(32.6) | <0.001 |
| High school | 2,930(29.5) | 1,173(28.5) | 1,757(30.1) | |
| ≥College | 3,354(32.8) | 1,112(26.2) | 2,242(37.2) | |
| Income | ||||
| Low | 2,511(24.7) | 1,121(27.1) | 1,390(23.0) | <0.001 |
| Middle | 5,134(50.2) | 2,095(49.6) | 3,039(50.6) | |
| High | 2,501(25.2) | 950(23.3) | 1,551(26.4) | |
| Smoking | ||||
| No | 6,130(61.7) | 2,220(54.5) | 3,910(66.6) | <0.001 |
| Yes | 4,016(38.3) | 1,946(45.5) | 2,070(33.4) | |
| Drinking | ||||
| No | 5,854(58.0) | 2,330(55.9) | 3,524(59.3) | <0.001 |
| Yes | 4,292(42.0) | 1,836(44.1) | 2,456(40.7) | |
| Chronic disease | ||||
| No | 5,915(58.5) | 2,136(51.1) | 3,779(63.5) | <0.001 |
| Yes | 4,231(41.5) | 2,030(48.9) | 2,201(36.5) | |
| Frequency of daily tooth brushing | ||||
| ≤1 | 1,075(10.1) | 548(12.8) | 527(8.2) | <0.001 |
| 2 | 3,958(38.7) | 1,707(40.8) | 2,251(37.3) | |
| ≥3 | 5,113(51.3) | 1,911(46.4) | 3,202(54.5) | |
| Unmet dental treatment needs | ||||
| No | 7,346(72.7) | 2,867(69.2) | 4,479(75.0) | <0.001 |
| Yes | 2,800(27.3) | 1,299(30.8) | 1,501(25.0) | |
| Oral health examination in the past year | ||||
| No | 6,427(62.9) | 2,813(67.5) | 3,614(59.8) | <0.001 |
| Yes | 3,719(37.1) | 1,353(32.5) | 2,366(40.2) | |
*by complex sample chi square test
Analysis of clinical and subjective oral health status according to health related behaviors showed significant differences across all variables, including chronic disease, frequency of daily toothbrushing, unmet dental treatment needs, oral health examination in the past year, and mental health consultation in the past year. Participants without chronic disease showed a higher proportion of mismatch (64.8%) compared with those who had chronic disease (52.6%) (p<0.001). Regarding frequency of daily toothbrushing, the proportions of mismatch were 63.6% for ≥3 times, 57.5% for twice, and 48.8% for ≤1 time, indicating that higher brushing frequency was associated with a greater likelihood of mismatch (p<0.001). Participants without unmet dental treatment needs showed a higher proportion of mismatch (75.0%) (p<0.001), and those who had not undergone an oral health examination in the past year also showed a higher proportion of mismatch (61.7%) (p<0.001). Participants who had received mental health consultation in the past year showed a higher proportion of mismatch (67.4%) (p=0.033) <Table 2>.
Table 2. Match and mismatch between clinical and subjective periodontal status according to health related behaviors [Unit: N(%)]
| Characteristics | Total | Clinical and subjective oral health status | p* | |
|---|---|---|---|---|
| Match | Mismatch | |||
| Total | 10,146(100.0) | 4,166(40.3) | 5,980(59.7) | |
| Chronic disease | ||||
| No | 5,915(58.5) | 2,136(35.2) | 3,779(64.8) | <0.001 |
| Yes | 4,231(41.5) | 2,030(47.4) | 2,201(52.6) | |
| Frequency of daily tooth brushing | ||||
| ≤1 | 1,075(10.1) | 548(51.2) | 527(48.8) | <0.001 |
| 2 | 3,958(38.7) | 1,707(42.5) | 2,251(57.5) | |
| ≥3 | 5,113(51.3) | 1,911(36.4) | 3,202(63.6) | |
| Unmet dental treatment needs | ||||
| No | 7,346(72.7) | 2,867(38.3) | 4,479(61.7) | <0.001 |
| Yes | 2,800(27.3) | 1,299(45.4) | 1,501(54.6) | |
| Oral health examination in the past year | ||||
| No | 6,427(62.9) | 2,813(43.2) | 3,614(56.8) | <0.001 |
| Yes | 3,719(37.1) | 1,353(35.2) | 2,366(64.8) | |
| Mental health consultation in the past year | ||||
| No | 4,069(40.5) | 5,783(59.5) | 0.033 | |
| Yes | 97(32.6) | 197(67.4) | ||
*by complex sample chi square test
The independent effects of various factors on the mismatch between clinical and subjective oral health status were as follows. Individuals who had received mental health counseling within the past year showed a higher likelihood of exhibiting a discrepancy than those who had not, with an odds ratio (OR) of 1.496 (95% CI: 1.496–1.072). Among general characteristics, males had a significantly lower likelihood of discrepancy compared with females (OR=0.598). Age was also negatively associated with mismatch, with each one year increase corresponding to a 0.982 fold lower likelihood of discrepancy (OR=0.982).
Regarding educational level, individuals with a college degree or higher had a lower likelihood of discrepancy than those with a middle school education or less (OR=0.702). Smokers also showed a lower likelihood of mismatch compared with non-smokers (OR=0.847).
Among health related behavioral variables, individuals with chronic diseases had a lower likelihood of discrepancy than those without chronic diseases (OR=0.849). Likewise, those with unmet dental treatment needs showed a lower likelihood of discrepancy compared with those without unmet needs (OR=0.771). Meanwhile, individuals who had undergone an oral health examination within the past year had a higher likelihood of discrepancy than those who had not (OR=1.164) <Table 3>.
Table 3. Multivariable logistic regression analysis of factors associated with mismatch between clinical and subjective oral health status
| Factors | Mismatch between clinical and subjective oral health status | |
|---|---|---|
| OR(95% CI) | p* | |
| Mental health consultation in the past year | ||
| No | 1.000 | |
| Yes | 1.496(1.496-1.072) | 0.018 |
| Gender | ||
| Female | 1.000 | |
| Male | 0.598(0.520-0.687) | <0.001 |
| Age (yr) | 0.982(0.977-0.987) | <0.001 |
| Education | ||
| ≤Middle school | 1.000 | |
| High school | 0.871(0.755-1.005) | 0.058 |
| ≥College | 0.702(0.597-0.824) | <0.001 |
| Income | ||
| Low | 1.000 | |
| Middle | 0.897(0.798-1.008) | 0.067 |
| High | 0.876(0.744-1.032) | 0.113 |
| Smoking | ||
| No | 1.000 | |
| Yes | 0.847(0.733-0.978) | 0.024 |
| Drinking | ||
| No | 1.000 | |
| Yes | 0.926(0.834-1.029) | 0.155 |
| Chronic disease | ||
| No | 1.000 | |
| Yes | 0.849(0.758-0.951) | <0.001 |
| Frequency of daily tooth brushing | 1.026(0.978-1.076) | 0.300 |
| Unmet dental treatment needs | ||
| No | 1.000 | |
| Yes | 0.771(0.690-0.862) | <0.001 |
| Oral health examination in the past year | ||
| No | 1.000 | |
| Yes | 1.164(1.051-1.289) | <0.001 |
OR: odd ratio; CI: confidence interval
This study analyzed data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018). The analysis aimed to examine the prevalence of mismatch between clinical periodontal status and subjective oral health perception among Korean adults aged 35 years and older, and to identify factors associated with this discrepancy. The findings revealed that 59.7% of participants demonstrated a mismatch between their clinical periodontal condition and perceived oral health status. It is indicating that a substantial proportion of adults do not accurately recognize their periodontal health. This pattern is consistent with previous studies reporting gaps between subjective oral health perception and objective clinical indicators [7,8,11]. In the present study, the mismatch group showed significant differences from the match group across most sociodemographic and behavioral characteristics, including sex, age, education, income, smoking, drinking, chronic disease status, and oral health behaviors.
The multivariable logistic regression analysis identified several factors associated with this mismatch. First, adults who had received mental health counseling during the past year had a 1.496-fold higher likelihood of mismatch compared with those without such experience (p=0.018). This finding suggests that mental health status is an important independent determinant of inaccurate oral health perception. It is consistent with previous evidence indicating that stress, anxiety, or depressive symptoms may distort subjective health evaluations [16,21,22]. Clinically, this may manifest as mismatch wherein individuals with relatively healthy periodontal status perceive their oral health as poor due to psychological influences. These results highlight the need for patient education strategies that incorporate psychological considerations in clinical practice.
Second, individuals who reported undergoing a dental check-up within the past year exhibited a 1.164-fold higher probability of mismatch (p<0.001) than those without such experience. This unexpected result suggests that dental examinations do not necessarily improve patient’s understanding of their periodontal health. Possible explanations include insufficient explanation of asymptomatic early stage periodontal disease or a lack of patient comprehension regarding the clinical information provided [20]. Therefore, dental hygienists should reinforce post examination communication by delivering clear, personalized, and literacy appropriate information to enhance patient’s understanding of their periodontal status.
Conversely, several characteristics were associated with reduced mismatch. Men were less likely to experience mismatch than women (OR=0.598, p<0.001), consistent with literature suggesting that women tend to be more sensitive or pessimistic in their subjective health assessments. Increasing age was associated with a gradual decline in mismatch (OR=0.982 per year, p<0.001), possibly reflecting greater exposure to symptoms and disease progression among older adults, resulting in more accurate recognition of their periodontal condition [12].
Among behavioral factors, smokers showed a lower likelihood of mismatch than non-smokers (OR=0.847, p=0.024). Individuals with chronic disease also had lower mismatch odds (OR=0.849, p<0.001), suggesting that those with systemic conditions may possess greater health awareness and thus more accurate oral health perception. Notably, unmet dental needs were strongly associated with lower mismatch (OR=0.771, p<0.001), indicating that individuals who perceive a need for dental treatment frequently present with actual clinical periodontal problems, resulting in more accurate perception.
Overall, these results demonstrate that subjective oral health perception does not adequately reflect clinical periodontal status among a large proportion of Korean adults. The findings also indicate that mismatch is particularly prevalent among individuals with poor mental health or those who undergo routine dental check-ups, highlighting the need for enhanced patient provider communication in these groups. Dental hygienists should assess patients’ subjective oral health beliefs and utilize objective clinical data such as intraoral photographs, radiographs, and periodontal probing depths to provide clear explanations and strengthen patient understanding of the necessity of preventive care.
This study contributes to the literature by identifying sociopsychological and behavioral determinants of mismatch between perceived and clinical periodontal health, offering implications for both clinical practice and public health policy. However, several limitations should be noted. First, this study used data from the Seventh Korea National Health and Nutrition Examination Survey (2016–2018), which represents the most recent cycle that included nationwide clinical periodontal examinations. Because periodontal clinical measurements have not been publicly released in KNHANES since 2016–2018, more up to date nationally representative periodontal data were not available. Although these data are approximately 8–10 years old, they remain the latest and only comprehensive source of nationwide periodontal clinical indicators and are therefore appropriate for examining factors associated with mismatch between clinical periodontal status and subjective perception. In addition, the cross sectional design of KNHANES limits the ability to infer causal relationships between the identified factors and the mismatch. Together, these structural constraints of the dataset should be considered when interpreting the study findings. Second, subjective oral health perception was dichotomized into “good” and “poor,” which may not fully capture the nuanced perceptions of those responding “average.” Third, this study did not include other subjective oral health related variables such as toothache, chewing discomfort, perceived gingival bleeding, or OHIP scores. Future studies should incorporate these variables to provide a more comprehensive understanding of the mismatch between subjective and clinical periodontal status. Fourth, periodontal status was assessed using the Community Periodontal Index, which evaluates only index teeth and may therefore underestimate the true severity of periodontal disease. In addition, grouping CPI codes 0–2 as”no disease”may oversimplify early or mild periodontal conditions. These structural limitations of CPI should be taken into account when interpreting the findings of this study. Fifth, because this study employed a cross sectional design, causal inferences cannot be made regarding the association between oral health examination and the likelihood of mismatch. Rather, possible explanation such as limited understanding of dental examination results, insufficient awareness of early asymptomatic periodontal conditions should be considered. Longitudinal or qualitative research is needed to clarify these mechanisms.
Future research should employ refined classifications of mismatch types and investigate the underlying psychological and behavioral mechanisms contributing to these discrepancies. Additionally, intervention studies evaluating communication strategies designed to reduce mismatch may provide evidence for developing patient centered periodontal health education and public oral health policies aimed at improving preventive care engagement and health equity.
This study examined 10,146 adults aged 35 years and older who participated in the Seventh Korea National Health and Nutrition Examination Survey (2016–2018) to identify factors associated with the mismatch between clinical periodontal status (CPI) and subjective oral health perception.
1. A total of 59.7% of participants demonstrated a mismatch between their clinical periodontal condition and perceived oral health status, indicating that Korean adults generally have limited awareness of their actual periodontal health.
2. Multivariable logistic regression analysis revealed that mismatch was significantly associated with several sociodemographic and behavioral characteristics, including female, younger age, non-smoking status, absence of chronic disease, and absence of unmet dental needs.
3. Notably, individuals who had undergone a dental check-up within the past year (OR=1.164, 95% CI: 1.051–1.289) and those with a history of mental health counseling (OR=1.496, 95% CI: 1.072–2.086) showed a significantly higher likelihood of mismatch. These findings suggest that routine dental examinations or mental health challenges may hinder accurate recognition of one’s periodontal condition.
Overall, the results highlight the importance of assessing both subjective perception and psychological characteristics when planning dental hygiene interventions for periodontal disease prevention and management. Individuals with poor mental health or those who regularly undergo dental examinations represent high risk groups for mismatch; therefore, enhanced explanation using objective clinical information, personalized communication strategies, and educational approaches to improve oral health literacy are needed to promote accurate health perception. This study provides foundational evidence to inform future public oral health strategies aimed at improving periodontal disease prevention and advancing health equity.
Conceptualization: HJ Cho, IS Chang, IS Jung; Data collection: SH Lee, EJ Choi; Formal analysis: YS Jung, SH Lee; Writing-original draft: SH Lee, EJ Choi; Writing-review&editing: HJ Cho, IS Chang, YS Jung
YS Jung is a member of the Editorial Committee of the Journal of the Korean Society of Dental Hygiene, but was not involved in the review process of this manuscript. The authors declare no other conflicts of interest.
None.
Non-human or animal research.
The data are held by the corresponding author and are available upon request if needed.
None.
Wu S, Wang R, Zhao Y, Ma X, Wu M, Yan X, et al. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health 2013;13:320. https://doi.org/10.1186/1471-2458-13-320.
Fall A, Migot-Nabias F, Zidi N. Empirical Analysis of Health Assessment Objective and Subjective Methods on the Determinants of Health. Front Public Health 2022;10:796937. https://doi.org/10.3389/fpubh.2022.796937.
Bombak AE. Self-rated health and public health: a critical perspective. Front Public Health 2013;1:15. https://doi.org/10.3389/fpubh.2013.00015.
Ruzicka M, Ibarra Fonseca GJ, Sachenbacher S, Heimkes F, Grosse-Wentrup F, Wunderlich N, et al. Substantial differences in perception of disease severity between post COVID-19 patients, internists, and psychiatrists or psychologists: the Health Perception Gap and its clinical implications. Eur Arch Psychiatry Clin Neurosci 2024;274(8):2015-24. https://doi.org/10.1007/s00406-023-01700-z.
Calvey B, McHugh Power J, Maguire R, Welmer AK, Calderón-Larrañaga A. How do discrepancies between subjective and objective health predict the risk of injurious falls? a study of community-dwelling Swedish older adults. J Am Med Dir Assoc 2024;25(8):105072. https://doi.org/10.1016/j.jamda.2024.105072.
Jung NH, Lee CY. Subjective and objective health according to the characteristics of older adults: using data from a national survey of older Koreans. Medicine 2024;103(47):e40633. https://doi.org/10.1097/MD.0000000000040633.
Rana BK, Kiyani A, Hassan S, Masood R, Javed MQ, Abulhamael AM, et al. Assessment of treatment needs, barriers, and self-perception regarding oral health among female university students: a cross-sectional study. BMC Oral Health 2024;24(1):883. https://doi.org/10.1186/s12903-024-04658-z.
Maille G, Saliba-Serre B, Ferrandez AM, Ruquet M. Objective and perceived oral health status of elderly nursing home residents: a local survey in southern France. Clin Interv Aging 2019;14:1141-51. https://doi.org/10.2147/CIA.S204533.
Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primers 2017;3:17038. https://doi.org/10.1038/nrdp.2017.38.
Tervonen T, Knuuttila M. Awareness of dental disorders and discrepancy between “objective” and “subjective” dental treatment needs. Community Dent Oral Epidemiol 1988;16(6):345-8. https://doi.org/10.1111/j.1600-0528.1988.tb00579.x.
Vered Y, Sgan-Cohen HD. Self-perceived and clinically diagnosed dental and periodontal health status among young adults and their implications for epidemiological surveys. BMC Oral Health 2003;3(1):3. https://doi.org/10.1186/1472-6831-3-3.
Romano F, Perotto S, Bianco L, Parducci F, Mariani GM, Aimetti M. Self-perception of periodontal health and associated factors: a crosssectional population-based study. Int J Environ Res Public Health 2020;17(8):2758. https://doi.org/10.3390/ijerph17082758.
Olutola BG, Ayo-Yusuf OA. Socio-environmental factors associated with self-rated oral health in South Africa: a multilevel effects model. Int J Environ Res Public Health 2012;9(10):3465-83. https://doi.org/10.3390/ijerph9103465.
Kotha SB, Chaudhary M, Terkawi S, Ahmed M, Ghabban SN, Fernandez RAA. Correlation of perceived self-rated oral health status with various dental health and awareness factors. J Int Soc Prev Community Dent 2017;7(S2):S119-24. https://doi.org/10.4103/jispcd.JISPCD_304_17.
Ghanem AS, Móré M, Nagy AC. Assessing the impact of sociodemographic and lifestyle factors on oral health: a cross-sectional study in the Hungarian population. Front Public Health 2023;11:1276758. https://doi.org/10.3389/fpubh.2023.1276758.
Nordin M, Sundström A, Hakelind C, Nordin S. Self-rated health and its bidirectional relationship with burnout, sleep quality and somatic symptoms in a general adult population. BMC Public Health 2024;24(1):2094. https://doi.org/10.1186/s12889-024-19325-9.
Shields GS, Fassett-Carman A, Gray ZJ, Gonzales JE, Snyder HR, Slavich GM. Why is subjective stress severity a stronger predictor of health than stressor exposure? A preregistered two-study test of two hypotheses. Stress Health 2023;39(1):87-102. https://doi.org/10.1002/smi.3165.
Ball J, Darby I. Mental health and periodontal and peri-implant diseases. Periodontol 2000 2022;90(1):106-24. https://doi.org/10.1111/prd.12452.
Alghanem J, Haque S, Ababneh K, Fakhoury HMA, Zangiabadi S, Tamim H. Poor perceived oral health is associated with adverse mental health outcomes among Syrian refugees in Canada. PLOS Glob Public Health 2024;4(11):e0003824. https://doi.org/10.1371/journal.pgph.0003824.
Chen MY. Misperception of oral health among adults in rural areas: a fundamental but neglected issue in primary healthcare. Int J Environ Res Public Health 2018;15(10):2187. https://doi.org/10.3390/ijerph15102187.
Herbert C. Oral health and mental health in healthy adults, a topic of primary prevention and health care, empirical results from two online studies. Curr Psychol 2023;42:32110-24. https://doi.org/10.1007/s12144-022-04121-8.
Nangle MR, Manchery N, Swayne A, Boocock H, Blum S, Henry JD. Oral health-related quality of life is more strongly correlated with mental health than with oral health in relapsing-remitting multiple sclerosis. J Oral Rehabil 2023;50(1):62-8. https://doi.org/10.1111/joor.13387.