
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Elastria Widita1![]() , Budi Rodestawati2
, Budi Rodestawati2![]() , Lisdrianto Hanindriyo2
, Lisdrianto Hanindriyo2![]() , Christia Aye Waindy Vega2
, Christia Aye Waindy Vega2![]() , Bekti Nur’aini2
, Bekti Nur’aini2![]() , Fimma Naritasari1
, Fimma Naritasari1![]() , Dewi Agustina1
, Dewi Agustina1![]()
1Department of Oral Medicine, Faculty of Dentistry, Universitas Gadjah Mada
2Department of Preventive Dentistry and Dental Public Health, Faculty of Dentistry, Universitas Gadjah Mada
Correspondence to Elastria Widita, Department of Oral Medicine, Faculty of Dentistry, Universitas Gadjah Mada, Jalan Denta No. 1, Sekip Utara, Yogyakarta 55281, Indonesia. Tel: +6281802646660, E-mail: elastria_widita@ugm.ac.id
Volume 26, Number 1, Pages 23–32, February 2026.
J Korean Soc Dent Hyg 2026;26(1):23–32. https://doi.org/10.13065/jksdh.2026.26.1.3
Received on November 24, 2025, Revised on December 26, 2025, Accepted on February 02, 2026, Published on February 28, 2026.
Copyright © 2026 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: This study aimed to examine the association between periodontal disease and metabolic syndrome (MetS) in older adults. Methods: This cross-sectional study enrolled 122 older adults aged ≥ 60 years living in Yogyakarta, Indonesia. Periodontal disease was assessed based on the number of sites of probing pocket depth (PPD) and clinical attachment level (CAL). Five MetS components were assessed: obesity, elevated blood pressure, dyslipidemia, hypertriglyceridemia, and hyperglycemia. Older adults with abdominal obesity and at least two additional positive components were classified as having MetS. Logistic regression analysis was used to determine the association between periodontal disease and MetS, after adjusting for covariates. Results: Twenty-three percent of the participants had three or more positive MetS components. A greater number of sites with PPD ≥ 4 mm and CAL ≥ 9 mm was significantly associated with MetS (p<0.05). PPD and CAL were analyzed using separate multivariate models. The number of sites with PPD ≥ 4 mm was significantly associated with MetS (OR=1.04; 95% CI=1.01–1.07), while a higher number of sites with CAL ≥ 9 mm was also associated with MetS (OR=1.19; 95% CI=1.06–1.32). Conclusions: The present findings demonstrate an association between periodontal disease and MetS in older adults. While statistically significant, this relationship should be interpreted with caution given the cross-sectional design. Longitudinal studies are needed to clarify the temporal pathways linking periodontal status and metabolic health.
Clinical attachment level, Metabolic syndrome, Older adults, Pocket depth
The demographic transition associated with changes in disease patterns and increased life expectancy is a global phenomenon observed not only in industrialized but also in developing countries [1,2]. Yogyakarta has the highest life expectancy in Indonesia and is expected to become one of the aging provinces, with more than 10% of the population aged 65 years and over by 2035 [3]. In Indonesia, rapid population aging is accompanied by an increasing burden of chronic non-communicable diseases, making it important to identify factors that may contribute to cardiovascular risk among older adults. Older adults are at risk of developing chronic conditions, including cardiovascular and periodontal disease [4–6]. The incidence of cardiovascular disease has been reported to increase in individuals with metabolic syndrome (MetS), which is more prevalent among older adults [7–11].
MetS is characterized by a clustering metabolic disorders, including elevated blood pressure, increased waist circumference, low HDL cholesterol, high triglycerides, and hyperglycemia [12]. The components of metabolic syndrome have been reported to be associated with periodontal disease [13,14]. Periodontal disease is characterized by pathological loss of the supportive connective tissue and alveolar bone surrounding the teeth, resulting from periodontal pathogen infection [15]. The prevalence, extent, and severity of periodontal disease have been associated with MetS [13]. A current systematic review concluded that patients with periodontal disease have a higher risk of MetS [16]. Periodontal disease and MetS are multifactorial conditions sharing common inflammatory pathways. Elevated levels of inflammatory mediators such as C-reactive protein (CRP), interleukin-6 (IL6), and tumor necrosis factor-α (TNF-α) have been reported among people with MetS [17]. Elevated levels of these inflammatory markers have also been observed in individual with periodontal disease [18,19]. However, data on the association between periodontal disease and MetS among community-dwelling older adults in Southeast Asia, particularly Indonesia, remain limited. Addressing this gap may help clarify whether this association is also observed in aging population in upper- and middle-income settings.
In view of these observation, investigating the relationship between periodontal disease and MetS is essential to improve understanding of how periodontal disease may relate to systemic health in older adults. The aim of this cross-sectional study was to examine the association between periodontal disease and MetS among older adults living in Yogyakarta, Indonesia.
We conducted a community-based cross-sectional study in 2018 among older adults residing in Yogyakarta, Indonesia. Participants were recruited from five community health stations for older adults (Posyandu Lansia). The health stations were in the province of Daerah Istimewa Yogyakarta and were randomly selected. The sample size was determined using G*Power software (ver. 3.1.9.7; Heinrich Heine University Düsseldorf, Düsseldorf, Germany), assuming an odds ratio of 2.2 for the association between periodontal disease and MetS, a two-sided α of 0.05, power of 95% and the logistic regression as the main analysis. The minimum required sample size was 117 participants; we invited 150 to account for potential non-response. Letters of invitation to this survey were sent to 30 randomly selected participants from members of each Posyandu Lansia (n=150). Subjects aged 60 years and older were selected according to the inclusion and exclusion criteria. They were Yogyakarta residents, who underwent full-mouth periodontal examination. Older adults who were in good health, dentulous and able to communicate were included in this study, while individuals who were suffering from severe infections, were hospitalized and edentulous were excluded from this study.
The study protocol was reviewed and approved by the Medical and Health Research Ethics Committee (MHERC), Faculty of Medicine, Universitas Gadjah Mada, and Dr. Sardjito General Hospital (KE/FK/0939/EC/2018). All study procedures were conducted in accordance with the Declaration of Helsinki (revised in 2000), and the rights, safety, and confidentiality of all participants were strictly protected. We adhered to the STROBE guidelines for reporting observational studies involving human participants [20]. All participants agreed to undergo all protocols and provided written informed consent prior to participation.
The intraoral examination included measurement of periodontal conditions and number of present teeth. The number of teeth was counted as the total remaining teeth including third molars. Periodontal disease was assessed using the number of sites of probing pocket depth (PPD) and clinical attachment level (CAL) as clinical parameter for periodontal disease, which provide more precise representation of the extent of periodontal diseases [21]. Periodontal examinations were conducted by five trained dentists at six sites around each tooth (mesio-buccal, mid-buccal, disto-buccal, mesio-lingual, mid-lingual/mid-palatal, and distolingual). Probing was performed using a blunt rounded tip probe (548/1 Medesy Probe, Italy) and measurement were rounded to the nearest whole millimeter. Examiners calibration was performed prior to data collection using volunteer patients at the University Dental Hospital, Universitas Gadjah Mada. Intra-examiner reliability was assessed through repeated periodontal measurements performed by the same examiner at different time points, whereas inter-examiner reliability was evaluated by comparing measurements obtained by different examiners. Agreement for categorical periodontal measurements was evaluated using kappa statistics, which are appropriate for assessing consistency beyond chance in categorized clinical parameters such as PPD and CAL thresholds. To minimize information bias, all clinical measurements were obtained using standardized protocols. The kappa values ranged from 0.75 to 0.90 for PPD and from 0.65 to 0.80 for CAL, indicating substantial to almost perfect agreement.
Anthropometric evaluation, blood pressure (BP) evaluation, laboratory procedure analysis and interview were used in this study. Anthropometric evaluation was calculated through body mass index (BMI) by measuring the height and weight of respondents. Waist circumference was measured with a soft tape on standing participants midway between the lowest rib and the iliac crest. The recordings of BP were obtained from the right arm of the participants in a sitting position after five minutes of rest.
Fasting blood samples were drawn for the measurement of hemoglobin A1c (HbA1c), hsCRP, albumin, calcium and lipid profile including low-density lipoprotein cholesterol (LDL), high-density lipoprotein cholesterol (HDL), triglyceride (TG), total cholesterol (TC). Samples were drawn by our certified health professionals and sent to our clinical laboratory Academic University Hospital, UGM. HbA1c was selected as a glycemic indicator due to its clinical relevance in older adults and its practical utility in communitybased epidemiological studies, where fasting plasma glucose alone may underestimate dysglycaemia. HsCRP was included to account for systemic inflammation [22], serum albumin for chronic inflammation and nutritional status [23], and serum calcium for mineral and bone metabolism [24].
MetS was defined using ATP III–based criteria adapted for Asian populations [12,25], requiring the presence of three or more components: abdominal obesity (waist circumference>90 cm in men and >80 cm in women), hyperglycemia (HbA1c≥6.0% and/or antidiabetic medication), elevated BP (≥130/85 mmHg and/or antihypertensive medication), hypertriglyceridemia (≥150 mg/dL and/or lipid-lowering therapy), and reduced high-density lipoprotein cholesterol (<40 mg/dL in men and <50 mg/dL in women). This definition was selected to enable broader identification of metabolic risk in older Asian populations [26].
The data on medication history, exercise habits, smoking status, socio-economic status, and oral-health behaviors were collected by using a standardized questionnaire and face-to-face interview. Information of oral-health behavior including brushing frequency (<2 times/d or ≥2 times/d), and pattern of dental visit (regularly or episodically) were collected. Lower education was defined as school attendance <9 years. Physical activity was measured using International Physical Activity Questionnaire Short Form (IPAQSF) and categorized according to standard scoring protocols. While smoking status information was collected with those reporting any smoking history classified as smokers.
All calculations and statistical analysis were performed using the statistical software package for windows version (ver. 22.0; IBM Corp. Armonk, NY, USA). P values of less than 0.05 were considered statistically significant. Characteristics of subjects were described using frequency distribution for categorical variables and the mean+standard deviation (SD) for continuous variables. Comparison between participants with and without MetS were conducted using t-test, and χ2 test, as appropriate. The association between MetS (dependent variable) and periodontal diseases (independent variable) as main predictor was assessed by logistic regression analysis. Multivariable models were adjusted for sex, education, smoking status, brushing frequency, pattern of dental visits, physical activity, number of remaining teeth, hsCRP, albumin and calcium, selected a priori based on biological plausibility and previous literature. All covariates were measured concurrently with exposure and outcome variables and were included in the models as continuous variables.
Periodontal parameters included PPD and CAL. PPD≥4 mm and CAL≥9 mm were entered into the regression models because these two clinical parameters showed statistically significant associations with MetS in the bivariate analyses. Logistic regression was performed to estimate the independent associations between periodontal disease and MetS with adjustment for potential confounders. PPD and CAL were modeled as continuous variables, expressed as per one-site increase in the number of sites with PPD≥4 mm and CAL≥9 mm. The threshold of CAL≥9 mm was selected to represent severe periodontal destruction and advanced cumulative periodontal tissue loss rather than localized disease, consistent with its use in previous epidemiological studies. To avoid multicollinearity, the number of sites with PPD≥4 mm and number of sites with CAL≥9 mm were entered separately into the models. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test.
Of the 150 older adults invited, 135 agreed to participate. Ten participants were unable to attend the examination because of personal reason, including urgent family issues, sickness, or transportation problems, while three others were edentulous. Thus, a total of 122 dentate participants were included into the final analysis (Fig. 1).
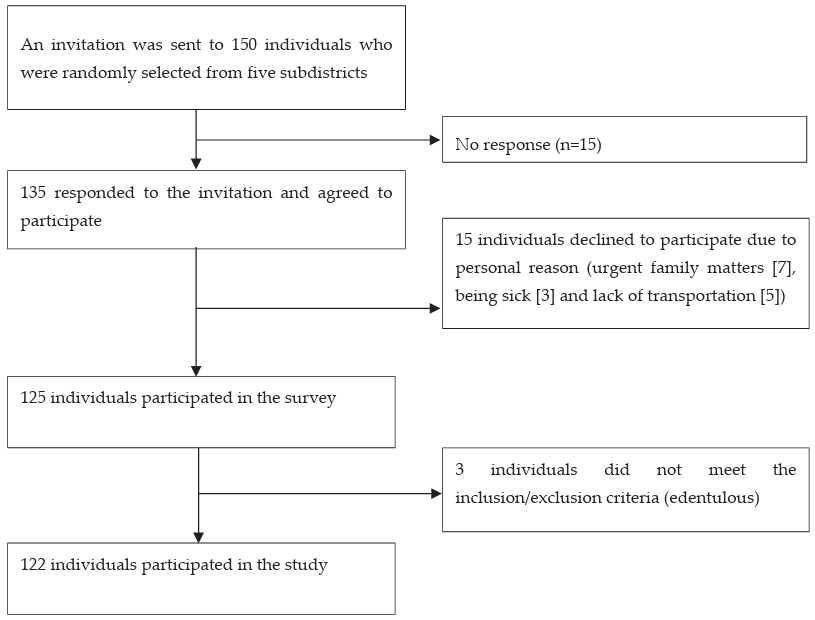
Fig. 1. Flow chart of the study
The prevalence of MetS in this sample was 23% (28/122). Behavioral and sociodemographic characteristics were broadly similar between MetS groups (Table 1). However, compared with those without MetS, participants with MetS had significantly lower HDL and higher mean triglyceride and HbA1c levels.
Table 1. Selected characteristic of the study participants without and with MetS
| Variables | MetS | p | |
|---|---|---|---|
| No (n=94) | Yes (n=28) | ||
| Mean±SD | |||
| Age (years) | 66.6±5.8 | 64.4±2.8 | 0.054* |
| Remaining teeth (n) | 19.4±6.2 | 18.5±5.9 | 0.502* |
| hsCRP (mg/dl) | 0.7±1.9 | 0.7±1.9 | 0.958* |
| Albumin (g/dl) | 4.4±0.52 | 4.4±0.2 | 0.648* |
| Calcium (mEq/L) | 8.9±1.7 | 9.0±1.7 | 0.970* |
| Creatinine | 0.9±0.2 | 0.9±0.3 | 0.109* |
| HDL (mg/dl) | 59.5±13.1 | 49.2±13.8 | <0.001* |
| LDL (mg/dl) | 132.8±34.6 | 140.1±36.9 | 0.334* |
| Triglycerides (mg/dl) | 104.4±44.4 | 184.1±152.84 | <0.001* |
| HbA1c (%) | 5.9±1.6 | 7.3±1.7 | <0.001* |
| n (%) | |||
| Gender | |||
| Women | 59.0 (48.4) | 21.0 (17.2) | 0.347** |
| Men | 35.0 (28.7) | 7.0 (5.7) | |
| Lower income | 52.0 (42.6) | 19.0 (15.6) | 0.238** |
| Lower education | 43.0 (35.3) | 10.0 (8.2) | 0.347** |
| Smoking | |||
| Nonsmoker | 76.0 (62.3) | 23.0 (18.9) | 0.878** |
| Smoker | 18.0 (14.8) | 5.0 (4.1) | |
| Physical activity | |||
| High | 35.0 (28.7) | 6.0 (4.9) | 0.260** |
| Moderate | 41.0 (33.6) | 14.0 (11.5) | |
| Low | 18.0 (14.8) | 8.0 (6.6) | |
| Visit dentist regularly | 22.0 (18.03) | 4.0 (3.2) | 0.375** |
| Tooth brushing ≥ 2 times/day | 19.0 (16.1) | 5.0 (4.1) | 0.783** |
MetS: metabolic syndrome; SD: standard deviation; hsCRP: high-sensitivity C-reactive protein; HDL: high-density lipoprotein; LDL: low-density lipoprotein; HbA1c: hemoglobin A1c
*by t-test, p<0.05; **by chi-square test, p<0.05
Regarding MetS components and related clinical characteristics (Table 2), 52 participants (42.6%) had elevated waist circumference and 44 (36.1%) had elevated HbA1c. Elevated BP was present in 31 participants (25.4%), reduced HDL cholesterol in 28 (23.0%), and increased triglyceride levels in 27 (22.1%). Eighteen participants (14.8%) were taking antidiabetic medications, 30 (24.6%) were on antihypertensive treatment, and 6 (4.9%) were receiving lipid-lowering medications.
Table 2. Anthropometric, clinical and relevant characteristics of MetS
| Variable | n (%) |
|---|---|
| Antidiabetic medications | 18.0 (14.8) |
| Antihypertension medications | 30.0 (24.6) |
| Antidyslipidemic medications | 6.0 (4.9) |
| Elevated waist circumference | 52.0 (42.6) |
| Elevated HbA1c | 44.0 (36.1) |
| Elevated blood pressure | 31.0 (25.4) |
| Reduce high-density lipoprotein | 28.0 (23.0) |
| Increased triglycerides level | 27.0 (22.1) |
MetS: metabolic syndrome; HbA1c: hemoglobin A1c
Full-mouth examination indicated a measurable site-level burden of periodontal disease in this community-dwelling older adults (Table 3). Mean PPD and CAL did not differ significantly between participants with and without MetS. However, those with MetS had a significantly higher number of sites with PPD≥4 mm and number of sites with CAL≥9 mm (p=0.031 and p=0.034, respectively), whereas no significant differences were observed for other PPD and CAL thresholds.
Table 3. Extent and severity of periodontal disease according to the participants without and with MetS
| Variables | MetS | p* | |
|---|---|---|---|
| No (n=94) | Yes (n=28) | ||
| Mean±SD | |||
| Average PPD | 1.8±0.9 | 1.7±0.8 | 0.574 |
| Average CAL | 1.8±1.8 | 1.9±1.4 | 0.889 |
| Number of sites PPD | |||
| PPD≥3 mm | 46.7±32.1 | 39.9±30.8 | 0.325 |
| PPD≥4 mm | 11.1±13.3 | 18.0±18.6 | 0.031 |
| PPD≥5 mm | 5.5±8.6 | 5.3±8.2 | 0.926 |
| PPD≥6 mm | 4.2±7.2 | 6.3±9.0 | 0.269 |
| Number of sites CAL | |||
| CAL≥3 mm | 31.2±23.2 | 32.7±19.7 | 0.753 |
| CAL≥4 mm | 22.1±21.7 | 22.4±19.7 | 0.953 |
| CAL≥5 mm | 17.1±20.2 | 17.5±19.3 | 0.917 |
| CAL≥6 mm | 12.2±18.3 | 12.2±18.3 | 0.823 |
| CAL≥9 mm | 2.1±3.6 | 5.1±6.8 | 0.034 |
MetS: metabolic syndrome; SD: standard deviation; PPD: probing pocket depth; CAL: clinical attachment level
*by chi-square test, p<0.05
As shown in Table 4, participants with hyperglycaemia and those with dyslipidaemia had significantly higher mean numbers of sites with CAL≥9 mm than those without these conditions (p=0.043 and p=0.011, respectively). In addition, the mean number of sites with CAL≥9 mm increased with the number of MetS components, and this association was statistically significant (p=0.003).
Table 4. Associations between the components of MetS and periodontal condition
| Variable | Sites with PPD ≥ 4 mm (n) | p* | Sites with CAL ≥ 9 mm (n) | p* | |
|---|---|---|---|---|---|
| Mean±SD | Mean±SD | ||||
| Abdominal obesity | No (72) | 10.9±12.7 | 0.136 | 2.1±3.5 | 0.054 |
| Yes (50) | 15.2±17.3 | 3.9±5.8 | |||
| Hypertension | No (47) | 10.6±11.9 | 0.230 | 1.9±3.8 | 0.067 |
| Yes (75) | 13.9±16.4 | 3.4±8.6 | |||
| Hyperglycemia | No (74) | 11.6±14.5 | 0.304 | 2.1±3.7 | 0.043 |
| Yes (48) | 14.4±15.5 | 3.8±5.7 | |||
| Dyslipidemia | No (80) | 10.9±12.3 | 0.120 | 1.8±7.9 | 0.011 |
| Yes (42) | 15.9±18.6 | 4.5±6.1 | |||
| MetS components | 1 (41) | 12.3±13.3 | 0.836 | 1.4±2.7 | 0.003 |
| 2 (31) | 12.8±15.9 | 0.948 | 3.9±4.7 | 0.138 | |
| 3 (34) | 15.7±17.7 | 0.165 | 4.4±6.3 | 0.056 | |
MetS: metabolic syndrome; PPD: probing pocket depth; CAL: clinical attachment level; SD: standard deviation
*by t-test, p<0.05
The association between periodontal disease and MetS was further examined using logistic regression analysis (Table 5). Two model were constructed, with the number of sites with PPD≥4 mm (Model 1) and the number of sites with CAL≥9 mm (Model 2) entered separately as indicators of periodontal disease extent. After adjustment for gender, education, smoking status, physical activity, pattern of dental visits, toothbrushing frequency, hsCRP, albumin, and calcium, a higher number of sites with PPD≥4 mm was significantly associated with increased odds of MetS (OR=1.04; 95% CI: 1.01–1.07; p=0.010). Similarly, a higher number of sites with CAL ≥9 mm was associated with increased odds of MetS (OR=1.19; 95% CI: 1.06–1.32; p=0.002).
Table 5. Associations between MetS and periodontal condition
| Variable | MetS (No; Yes) OR (95%CI) |
p* |
|---|---|---|
| Model 1 Sites with PPD≥4 mm (n) |
1.04 (1.01–1.07) | 0.010 |
| Model 2 Sites with CAL≥9 mm (n) |
1.19 (1.06–1.32) | 0.002 |
MetS: metabolic syndrome; OR: odds ratio; CI: confidence interval; PPD: probing pocket depth; CAL: clinical attachment loss * by logistic regression analysis, p<0.05
Adjusted for gender, smoking status, education status, physical activity, pattern of dental visit, toothbrushing, high-sensitivity C-reactive protein, albumin and calcium, number of remaining teeth.
In this study, an association was observed between periodontal disease and MetS among older adults in Yogyakarta, Indonesia after adjustment for potential confounders. A greater extent of periodontal disease, expressed as the number of sites with PPD≥4 mm and CAL≥9 mm, was significantly associated with the presence of MetS. Although the data were collected in 2018, the underlying biological mechanisms linking periodontal disease and MetS are unlikely to have changed over time [14,27], and the present dataset provides important baseline evidence from a rapidly aging population in Indonesia, where epidemiological data on periodontal–systemic associations remain limited. These findings add to the growing body of evidence suggesting a link between periodontal status and MetS in older population.
The findings of this study are consistent with previous reports showing that periodontal disease is associated with increased risk of MetS, and are further supported by recent large cohort studies and meta-analyses published between 2020 and 2024, which have confirmed a significant association between periodontitis and MetS across diverse populations [16]. Several biological mechanisms may underlie this association. Infections caused by gram-negative periodontal pathogens might stimulate the release of proinflammatory cytokines such as IL-1β and TNF-α [28]. A higher number of sites with PPD≥4 may reflect a larger burden of inflamed periodontal tissues and associated with increased levels of inflammatory mediators, whereas CAL≥9 mm reflects the cumulative destruction of periodontal tissue driven in part by TNF-α [29]. In addition, elevated levels of hsCRP, TNF-α, IL-1 and IL-6 have been reported in patients with MetS. Oxidative stress has also been proposed as key component underlying the association between periodontal disease and the MetS [30,31]. In the pro-inflammatory state, increased oxidative stress can occur in periodontal tissue, leading to DNA and protein damage [32]. This process may promote lipid peroxidation and oxidation of other enzymes and stimulates further production of pro-inflammatory mediators through activation of transcription factor related to tumor necrosis pathways.
It has been reported that individuals with periodontal disease exhibit increased levels of TNF-α and IL-1, which may contribute to MetS by interfering with lipase production and thereby adversely affecting the lipid profile [33,34]. Various pathogens included periodontal pathogens such as P. gingivalis, T. forsythia, and A. actinomycetemcomitans, have also been reported to induce changes in fat metabolism [35]. Other studies have hypothesized that recurrent bacteremia originating from periodontal lesions may alter in systemic markers in periodontitis and reinforce the close relationship between systemic disease and inflammation of the periodontal tissues [36]. Nevertheless, given the cross-sectional design of the present study, longitudinal and interventional studies are required to further clarify the temporal relationship and potential causality between periodontal disease and MetS.
The strengths of this study include the examination of a homogenous group of dentate Javanese older adults, which may reduce variability related to ethnic differences. However, several limitations should be considered when interpreting the findings. First, a potential selection bias cannot be excluded, as a participation in this study was voluntary and recruitment was conducted through community health stations. Older adults who were willing and able to participate may have been healthier, more health-conscious, or more socially engaged than non-participants, which may limit the representativeness of the sample and the generalizability of the findings to the broader older adult population. Second, the cross-sectional design precludes assessment of temporal relationships and causal inference between periodontal disease and MetS. Finally, information on important factors such as dietary intake, comprehensive comorbidity profiles, and detailed medical history was not collected. As a result, several potentially relevant confounding due to unmeasured factors dietary patterns and other comorbidities, cannot be ruled out.
1. A greater extent of periodontal disease was significantly associated with the presence of MetS among community-dwelling older adults.
2. These findings underscore the importance of maintaining oral health and regular dental care as part of comprehensive health management in aging populations with an increasing burden of MetS.
3. Longitudinal studies with larger and more diverse populations are needed to clarify the temporal relationship and potential causal pathways between periodontal disease and MetS.
Conceptualization: E Widita, B Rodestawati, L Hanindriyo, C Aye Waindy Vega, B Nur’aini; Data collection: E Widita, L Hanindriyo, D Agustina, F Naritasari; Formal analysis: E Widita, B Rodestawati, L Hanindriyo, C Aye Waindy Vega, B Nur’aini; Writing-original draft: E Widita, B Rodestawati, L Hanindriyo, C Aye Waindy Vega, Writing-review&editing: D Agustina , F Naritasari.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
This study was supported by grant from the Faculty of Dentistry Universitas Gadjah Mada. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
We conducted this study with approval from the Medical and Health Research Ethics Committee (MHERC), Faculty of Medicine, Universitas Gadjah Mada and Dr. Sardjito General Hospital (IRB approval no.: KE/FK/0939/EC/2018). Moreover, the study was conducted in accordance with the World Medical Association Declaration of Helsinki.
The data presented in this study are available on reasonable request from the corresponding author.
We thank to the Faculty of Dentistry, University Dental Hospital, Academic University Hospital from Universitas Gadjah Mada, Yogyakarta, Indonesia which facilitated the survey, and all the participants and investigators involved in the survey.
United Nations, Department of Economic and Social Affairs, Population Division. World population prospects 2023: summary of results. New York: United Nations; 2022.
United Nations, Department of Economic and Social Affairs, Population Division. World population ageing 2019-highlights. New York: United Nations; 2019.
BPS-Statistics Indonesia. Indonesia population projection 2010–2035. Jakarta: BPS-Statistics Indonesia; 2013: 458.
Lettino M, Mascherbauer J, Nordaby M, Ziegler A, Collet JP, Derumeaux G, et al. Cardiovascular disease in the elderly: proceedings of the European Society of Cardiology—Cardiovascular Round Table. Eur J Prev Cardiol 2022;29(10):1412–24. https://doi.org/10.1093/eurjpc/zwac033
Zhao C, Wong L, Zhu Q, Yang H. Prevalence and correlates of chronic diseases in an elderly population: a community-based survey in Haikou. PLoS One 2018;13(6):e0199006. https://doi.org/10.1371/journal.pone.0199006
Hanindriyo L, Widita E, Widyaningrum R, Priyono B, Agustina D. Influence of residential characteristics on the association between the oral health status and BMI of older adults in Indonesia. Gerodontology 2018;35(3):268–75. https://doi.org/10.1111/ger.12352
Tune JD, Goodwill AG, Sassoon DJ, Mather KJ. Cardiovascular consequences of metabolic syndrome. Transl Res 2017;183:57–70. https://doi.org/10.1016/j.trsl.2017.01.001
Suastika K, Dwipayana P, Saraswati IMR, Kuswardhani T, Astika N, Putrawan IB, et al. Relationship between age and metabolic disorders in the population of Bali. J Clin Gerontol Geriatr 2011;2(2):47–52. https://doi.org/10.1016/j.jcgg.2011.03.001
Kumar Karn S, Zhao F, Xu Y, Zhang Y, Zeng C, Shaikh II, et al. Metabolic syndrome with mortality and major adverse cardiovascular events in an elderly population. Front Endocrinol 2025;16:1570191. https://doi.org/10.3389/fendo.2025.1570191
Van Ancum JM, Jonkman NH, van Schoor NM, Tressel E, Meskers CGM, Pijnappels M, et al. Predictors of metabolic syndrome in community-dwelling older adults. PLoS One 2018;13(10):e0206424. https://doi.org/10.1371/journal.pone.0206424
Ranasinghe P, Mathangasinghe Y, Jayawardena R, Hills AP, Misra A. Prevalence and trends of metabolic syndrome among adults in the Asia-Pacific region: a systematic review. BMC Public Health 2017;17(1):101. https://doi.org/10.1186/s12889-017-4041-1
Grundy SM. Metabolic syndrome scientific statement by the American Heart Association and the National Heart, Lung, and Blood Institute. Arterioscler Thromb Vasc Biol 2005;25(11):2243–4. https://doi.org/10.1161/01.ATV.0000189155.75833.c7
Alhabashneh R, Khader Y, Herra Z, Asa’ad F, Assad F. The association between periodontal disease and metabolic syndrome among outpatients with diabetes in Jordan. J Diabetes Metab Disord 2015;14:67. https://doi.org/10.1186/s40200-015-0192-8
Pirih FQ, Monajemzadeh S, Singh N, Sinacola RS, Shin JM, Chen T, et al. Association between metabolic syndrome and periodontitis: the role of lipids, inflammatory cytokines, altered host response, and the microbiome. Periodontol 2000 2021;87(1):50–75. https://doi.org/10.1111/prd.12379
Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, et al. Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 2018;89(S1):S173–82. https://doi.org/10.1002/jper.17-0721
Gobin R, Tian D, Liu Q, Wang J. Periodontal diseases and the risk of metabolic syndrome: an updated systematic review and meta-analysis. Front Endocrinol 2020;11:336. https://doi.org/10.3389/fendo.2020.00336
Mohammadi M, Gozashti MH, Aghadavood M, Mehdizadeh MR, Hayatbakhsh MM. Clinical significance of serum IL-6 and TNF-α levels in patients with metabolic syndrome. Rep Biochem Mol Biol 2017;6(1):74–9. https://pubmed.ncbi.nlm.nih.gov/29090232/
Machado V, Botelho J, Escalda C, Hussain SB, Luthra S, Mascarenhas P, et al. Serum C-reactive protein and periodontitis: a systematic review and meta-analysis. Front Immunol 2021;12:706432. https://doi.org/10.3389/fimmu.2021.706432
Gani DK, Lakshmi D, Krishnan R, Emmadi P. Evaluation of C-reactive protein and interleukin-6 in the peripheral blood of patients with chronic periodontitis. J Indian Soc Periodontol 2009;13(2):69–74. https://doi.org/10.4103/0972-124X.55840
Malta M, Cardoso LO, Bastos FI, Magnanini MMF, da Silva CMFP. STROBE initiative: guidelines on reporting observational studies. Rev Saude Publica 2010;44:559–65. https://doi.org/10.1590/S0034-89102010000300021
Alawaji YN, Alshammari A, Mostafa N, Carvalho RM, Aleksejuniene J. Periodontal disease prevalence, extent, and risk associations in untreated individuals. Clin Exp Dent Res 2022;8(1):380–94. https://doi.org/10.1002/cre2.526
Paraskevas S, Huizinga JD, Loos BG. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J Clin Periodontol 2008;35(4):277–90. https://doi.org/10.1111/j.1600-051X.2007.01173.x
Li Y, Chen L, Yang X, Cui H, Li Z, Chen W, et al. Dynamic association of serum albumin changes with inflammation, nutritional status and clinical outcomes: a secondary analysis of a large prospective observational cohort study. Eur J Med Res 2025;30:679. https://doi.org/10.1186/s40001-025-02925-5
Amarasena N, Yoshihara A, Hirotomi T, Takano N, Miyazaki H. Association between serum calcium and periodontal disease progression in non-institutionalized elderly. Gerodontology 2008;25(4):245–50. https://doi.org/10.1111/j.1741-2358.2007.00211.x
Soewondo P, Purnamasari D, Oemardi M, Waspadji S, Soegondo S. Prevalence of metabolic syndrome using NCEP/ATP III criteria in Jakarta, Indonesia: the Jakarta primary non-communicable disease risk factors surveillance 2006. Acta Med Indones 2010;42(4):199–203. https://pubmed.ncbi.nlm.nih.gov/21063040/
Chen MM, Tsai AC. The effectiveness of IDF and ATP-III in identifying metabolic syndrome and the usefulness of these tools for health promotion in older Taiwanese. J Nutr Health Aging 2013;17(4):413–6. https://doi.org/10.1007/s12603-012-0440-2
Chairunisa F, Widita E, Thwin KM, Takehara S, Nohno K, Hanindriyo L, et al. Ten years’ evaluation of periodontal status and its changes among Japanese older adults. Spec Care Dentist 2024;44(6):1731–41. https://doi.org/10.1111/scd.13043
Graves DT, Cochran D. The contribution of interleukin-1 and tumor necrosis factor to periodontal tissue destruction. J Periodontol 2003;74(3):391–401. https://doi.org/10.1902/jop.2003.74.3.391
Di Benedetto A, Gigante I, Colucci S, Grano M. Periodontal disease: linking the primary inflammation to bone loss. J Immunol Res 2013;2013:503754. https://doi.org/10.1155/2013/503754
Bullon P, Morillo JM, Ramirez-Tortosa MC, Quiles JL, Newman HN, Battino M. Metabolic syndrome and periodontitis: is oxidative stress a common link? J Dent Res 2009;88(6):503–18. https://doi.org/10.1177/0022034509337479
Bullon P, Newman HN, Battino M. Obesity, diabetes mellitus, atherosclerosis and chronic periodontitis: a shared pathology via oxidative stress and mitochondrial dysfunction? Periodontol 2000 2014;64(1):139–53. https://doi.org/10.1111/j.1600-0757.2012.00455.x
Cekici A, Kantarci A, Hasturk H, Van Dyke TE. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000 2014;64(1):57–80. https://doi.org/10.1111/prd.12002
Abraham S, Premnath A, Arunima PR, Kassim RM. Critical appraisal of bidirectional relationship between periodontitis and hyperlipidemia. J Int Soc Prev Community Dent 2019;9(2):112–8. https://doi.org/10.4103/jispcd.JISPCD_316_18
Fu YW, Li XX, Xu HZ, Gong YQ, Yang Y. Effects of periodontal therapy on serum lipid profile and proinflammatory cytokines in patients with hyperlipidemia: a randomized controlled trial. Clin Oral Investig 2016;20:1263–9. https://doi.org/10.1007/s00784-015-1621-2
Leonov G, Varaeva Y, Livantsova E, Vasilyev A, Vladimirskaya O, Korotkova T, et al. Periodontal pathogens and obesity in the context of cardiovascular risks across age groups. Front Oral Health 2024;5:1488833. https://doi.org/10.3389/froh.2024.1488833
Ishikawa M, Yoshida K, Okamura H, Ochiai K, Takamura H, Fujiwara N, et al. Oral Porphyromonas gingivalis translocates to the liver and regulates hepatic glycogen synthesis through the Akt/GSK-3β signaling pathway. Biochim Biophys Acta 2013;1832(12):2035–43. https://doi.org/10.1016/j.bbadis.2013.07.012