
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Da-Jeong Kim1![]() , Ji-Young Lee2
, Ji-Young Lee2![]() , Yu-Rin Kim1
, Yu-Rin Kim1![]()
1Department of Dental Hygiene, Silla University
2Department of Dental Hygiene, Daedong University
Correspondence to Yu-Rin Kim, Department of Dental Hygiene, Silla University, 140 Baegyang-daero 700 beon-gil, Sasang-gu, Busan-si, 46958, Korea. Tel: +82-51-999-5592, Fax:+82-51-999-5745, E-mail: dbfls1712@hanmail.net
Volume 26, Number 2, Pages 179–91, April 2026.
J Korean Soc Dent Hyg 2026;26(2):179–91. https://doi.org/10.13065/jksdh.2026.26.2.5
Received on November 14, 2025, Revised on December 07, 2025, Accepted on December 24, 2025, Published on April 30, 2026.
Copyright © 2026 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Objectives: This study aimed to examine the mediating effect of health literacy on the relationship between generalized anxiety disorder (GAD) and problems with oral function among postmenopausal women in Korea. Data were obtained from the 2023 Korea National Health and Nutrition Examination Survey (KNHANES). The findings will inform strategies to enhance health literacy and promote sustainable oral health management. Methods: Data were obtained from the 2023 KNHANES, which was first year to include a health literacy index. Participants were divided into groups based on GAD status. Complex sampling analysis was conducted using IBM SPSS Statistics 21.0, and the PROCESS macro. Model 4. was applied to test the direct, indirect, and total effects of health literacy on the relationship between GAD and oral health problems. Results: After controlling for sociodemographic characteristics and comorbidities, health literacy was found to have a statistically significant mediating effect on the relationship between GAD and both chewing and speaking difficulties. Conclusions: GAD in postmenopausal women was associated with decreased oral function, and health literacy played a mediating role in alleviating this negative effect. It is recommended that oral health education programs that improve both anxiety management and health literacy are developed and implemented.
Health literacy, Korea, Menopause, Oral health, Women
Menopause constitutes a physiological transition in the female life course, marked by the progressive cessation of reproductive capacity and accompanied by a range of physical and psychological alterations resulting from diminished estrogen levels [1]. The reduction in estrogen triggers inflammatory processes, mucosal atrophy, and decreased salivary flow, thereby increasing the risk of oral pathologies such as xerostomia, taste dysfunction, and periodontal disease [2]. Additionally, the menopausal stage is identified as a critical period for mental health susceptibility, characterized by an elevated incidence of generalized anxiety disorder (GAD), which correlates with emotional distress, depressive symptoms, and disturbances in sleep patterns [3,4].
GAD is characterized by pervasive and difficult-to-manage anxiety and worry, which, together with associated somatic symptoms, significantly impair daily functioning [5]. The relationship between mental health and oral health has been extensively documented in the literature. Kisely [6] highlighted this connection by stating that “without mental health, there is no oral health,” thereby emphasizing the role of mental illness as a critical determinant of disparities in oral health outcomes. Moreover, research demonstrates that individuals diagnosed with anxiety and depressive disorders exhibit poorer oral health status—including a higher prevalence of dental caries, periodontal disease, and tooth loss—compared to those without such conditions. Anxiety has also been implicated in the etiology of various oral health problems, such as sleep bruxism and stress-related temporomandibular disorders [7–9].
The physiological mechanisms linking anxiety and oral health suggest that psychological stress reduces saliva production, impairs salivary immune function, and that stress-related behavioral patterns contribute to poor oral hygiene [10,11]. Moreover, recent studies have shown that functional disorders, such as temporomandibular disorders (TMD), tend to exacerbate in association with increased anxiety levels [9]. The relationship between mental health and oral health extends beyond psychological factors; it is proposed that stress-induced hormonal fluctuations and autonomic nervous system responses affect oral immune processes. Consequently, hormonal changes in postmenopausal women may interact with anxiety in a complex manner, thereby aggravating various oral health problems, including functional disorders. However, research on this topic in Korea remains notably limited.
Health literacy, defined as an individual’s ability to obtain, comprehend, evaluate, and utilize health-related information effectively, has recently been recognized as a crucial mediating factor in public health research [12]. This construct encompasses skills essential for acquiring, understanding, assessing, and applying health information, and is acknowledged as a significant social determinant that influences health behaviors, the use of preventive services, and self-management capacities, thereby substantially affecting individual health outcomes [12,13]. In the context of oral health, empirical studies have demonstrated that adults with low health literacy tend to have lower engagement with dental care services and poorer oral health status [14]. Recently, a health literacy measure was developed and incorporated into the Korea National Health and Nutrition Examination Survey (KNHANES) [15], enabling more objective evaluations in related studies. Health literacy is hypothesized to play a critical mediating role in the relationship between GAD and oral health complications. Specifically, women diagnosed with GAD who exhibit higher health literacy are better able to understand and apply pertinent oral health information, facilitating effective oral care practices that may prevent or alleviate oral functional impairments. However, there remains a notable lack of both domestic and international research investigating the mediating role of health literacy in the association between GAD and oral functional problems, particularly among postmenopausal women.
This study utilized data from the 2023 KNHANES to examine the mediating effect of health literacy on the relationship between GAD and oral function among postmenopausal women in Korea. The aim was to identify strategies to improve health literacy within this population and to provide foundational evidence to support effective oral health management.
This study employed data from the 2023 dataset, representing the second year of the ninth cycle, during which health literacy was newly integrated into the KNHANES. Since this survey is conducted directly by the government to promote public welfare, it received approval from the National Research Ethics Review Committee (ninth cycle, second year; approval number 2022-11-16-RA).
The KNHANES utilized a two-stage stratified cluster sampling design, with stratification based on administrative divisions (city/ province and dong/eup-myeon neighborhoods) and housing type (general housing versus apartments). Additional stratification criteria included residential area proportions, the age distribution of household heads, and the prevalence of single-person households [16]. In the second year of the ninth survey cycle (2023), a total of 9,825 individuals were surveyed, of whom 6,929 participated in at least one component of the health survey, health examination, or nutrition survey. After excluding cases with missing data on health literacy—a key mediator variable assessed via a self-administered health behavior questionnaire—1,569 postmenopausal women were identified from 5,323 respondents and included in the final analytical sample. The independent variables were divided into two groups: 668 participants diagnosed with GAD and 901 participants without such a diagnosis (without GAD group, Without_GAD) <Fig. 1>.
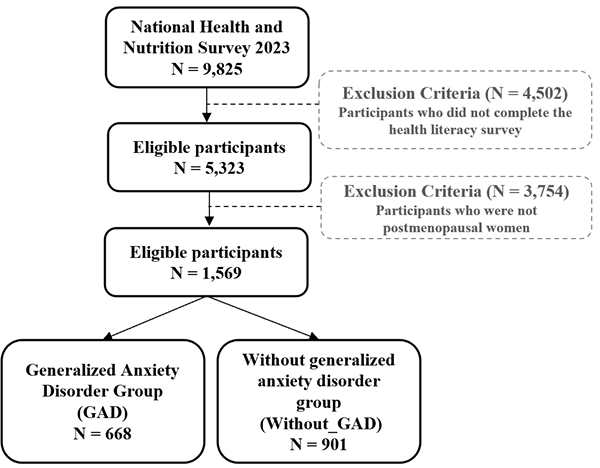
Fig. 1. Flow of study
Data on age, marital status, educational attainment, income level, employment status, smoking behavior, and alcohol consumption were obtained from the KNHANES. Age was categorized into four groups: 40–49 years, 50–59 years, 60–69 years, and 70 years or older. Marital status was dichotomized as married or unmarried. Educational attainment was classified into four levels: less than elementary school, middle school, high school, and college or higher. Income was divided into quintiles, labeled as lowest, lowermiddle, middle, upper-middle, and highest. Employment status was categorized as employed or unemployed. Smoking status was determined based on lifetime smoking history and classified into never smoked, fewer than five packs (fewer than 100 cigarettes), and five packs or more (100 cigarettes or more). Alcohol consumption frequency over the past year was categorized as at least once per month or less than once per month. The presence of comorbidities was identified based on current diagnoses of hypertension, dyslipidemia, and diabetes.
Oral health problems were evaluated through two indicators: challenges in chewing function and challenges in speaking function. These indicators were quantified using a 5-point Likert scale, with response options ranging from 1, indicating ‘very uncomfortable,’ to 5, indicating ‘not uncomfortable at all.’ For the current study, the scoring was reverse-coded so that higher values reflected increased severity of difficulty. The scale demonstrated acceptable internal consistency, as evidenced by a Cronbach’s alpha coefficient of 0.74.
In 2023, a health literacy assessment instrument—comprising both self-reported and knowledge-based components—was newly integrated as a performance indicator within the National Health Promotion Comprehensive Plan (Health Plan 2030) and administered to individuals aged 19 years and older [17]. The self-reported health literacy measure consisted of ten sub-items, each designed to evaluate the degree of difficulty respondents experience in understanding and utilizing health information in everyday contexts. Responses were rated on a four-point scale: 1 (“Not at all”), 2 (“Not really”), 3 (“Yes”), and 4 (“Very much”), with higher scores indicating greater health literacy. Among the tools utilized to evaluate comprehension of health literacy, knowledge-based instruments identified correct answers by means of passages and categorized participants as either correct or incorrect responders. In the analysis of mediation effects, a self-reported continuous variable was employed to serve as the mediator.
In the present study, GAD was incorporated as an independent variable during the eighth wave, corresponding to the third year (2023), with a focus on an adult cohort. GAD was evaluated through seven items that assessed the frequency of specific symptoms experienced by respondents over the preceding two weeks. These symptoms included: feeling nervous, anxious, or on edge; inability to stop or control worrying; excessive worry about various matters; difficulty relaxing; restlessness to the extent of being unable to remain still; increased irritability or annoyance; and feelings of fear as if something dreadful might occur. Participants’ responses were measured on a four-point Likert scale, where 0 represented “Not at all bothered,” 1 indicated “Bothered for several days,” 2 denoted “Bothered for more than seven days,” and 3 corresponded to “Bothered nearly every day.” For analytical purposes, the scores across the seven items were aggregated. Individuals with a cumulative score of zero were classified as not exhibiting GAD, whereas those with a total score of one or greater were categorized as having GAD.
The data analysis was performed using a complex sampling design that incorporated stratification variables, cluster variables, and sampling weights. All analyses were conducted with IBM SPSS Program (version 21.0; IBM Corp., Armonk, NY, USA). Within the total sample of 1,569 participants, comparisons of sociodemographic characteristics, overall health status, and oral health problems according to the presence or absence of GAD were conducted using complex sample design chi-square tests and complex sample linear regression analyses. To examine the direct, indirect, and total effects of the independent variable (GAD) on the dependent variable (oral health problems), with health literacy as a mediator, Hayes’ PROCESS macro Model 4 was employed [18] <Fig. 2>. The significance of the indirect effect was assessed using a 95% confidence interval derived from the distribution of indirect effects generated through 5,000 bootstrap samples. Potential confounding variables, including sociodemographic factors and comorbidities, were controlled for, and cases with missing data were excluded from the analyses. Sample sizes are presented as unweighted frequencies, and statistical significance was defined as 0.05.
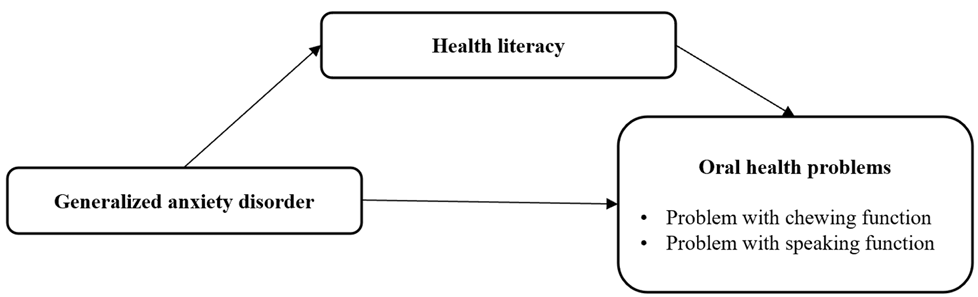
Fig. 2. Analysis model
<Table 1> presents the sociodemographic characteristics of postmenopausal women stratified by the presence or absence of GAD. In terms of age, the GAD was predominantly composed of women in their 50s (38.8%), whereas the Without_GAD group mainly consisted of women in their 60s (38.3%). Regarding educational attainment, the largest proportion within the GAD group were high school graduates (38.7%), while the Without_GAD group had the greatest representation among those with an education level of elementary school or below (34.0%). Analysis of income levels indicated that the GAD group had relatively higher proportions in the ‘lower-middle’ (23.6%) and ‘upper’ (22.2%) income categories, compared to the Without_GAD group, which exhibited the highest proportion in the ‘low’ income bracket (24.9%). Concerning employment status, a greater percentage of individuals in the GAD group were employed (52.5%), whereas the Without_GAD group had a higher proportion of unemployed individuals (53.7%). Both groups predominantly reported consuming fewer than one alcoholic beverage per month, with this difference reaching statistical significance (p<0.05).
Table 1. Differences in sociodemographic characteristics of postmenopausal women with generalized anxiety disorder [Unit: weighted N(%)]
| Characteristics | Division | Without_GAD (N=901) | GAD (N=668) | p |
|---|---|---|---|---|
| Age (yr) | 40-49 | 8(1.2) | 12(2.6) | <0.001 |
| 50-59 | 202(25.3) | 230(38.8) | ||
| 60-69 | 350(38.3) | 269(36.6) | ||
| 70≤ | 341(35.3) | 157(21.9) | ||
| Marriage status | Single | 20(2.5) | 20(3.6) | 0.241 |
| Married | 881(97.5) | 648(96.4) | ||
| Education level | ≤Elementary school | 327(34.0) | 177(24.1) | <0.001 |
| Middle school | 172(18.8) | 103(14.8) | ||
| High school | 266(31.7) | 243(38.7) | ||
| ≥University | 131(15.5) | 144(22.4) | ||
| Income level | Low | 240(24.9) | 137(19.0) | 0.015 |
| Low-middle | 205(21.5) | 160(23.6) | ||
| Middle | 169(18.7) | 111(16.6) | ||
| Middle-high | 144(18.0) | 119(18.6) | ||
| High | 138(16.9) | 140(22.2) | ||
| Economic activity status | Unemployed | 487(53.7) | 328(47.5) | 0.022 |
| Employed | 413(46.3) | 340(52.5) | ||
| Smoking | Non-smoking | 848(94.5) | 610(91.9) | 0.061 |
| <100 pieces | 2(0.1) | 0(0) | ||
| ≥100 pieces | 51(5.4) | 58(8.1) | ||
| Drinking | <1 month | 663(73.4) | 461(67.4) | 0.016 |
| ≥1 month | 238(26.6) | 207(32.6) | ||
| Comorbidities (yes, %) | High blood pressure | 369(97.5) | 246(97.1) | 0.805 |
| Dyslipidemia | 348(91.1) | 268(93.3) | 0.317 | |
| Diabetes | 137(97.9) | 101(99.3) | 0.337 |
*by complex sample chi-square test, p<0.05,
GAD: generalized anxiety disorder group; Without_GAD: without generalized anxiety disorder group
The findings regarding differences in health literacy based on the presence of GAD among postmenopausal women are summarized in <Table 2>. Concerning knowledge-based health literacy, the incidence of incorrect responses was significantly increased in the Without_GAD group relative to the GAD group (p<0.05). Conversely, no statistically significant differences were detected between the two groups in self-reported health literacy across all ten assessed items.
Table 2. Differences in health literacy in postmenopausal women with generalized anxiety disorder (Unit: Mean±SD)
| Characteristics | Division | Without_GAD (N=804) | GAD (N=611) | p |
|---|---|---|---|---|
| Knowledge type* | Incorrect answer group | 475 (58.2) | 295 (47.3) | <0.001 |
| Correct answer group | 329 (41.8) | 316 (52.7) | ||
| Self-reported type† | 1. Can you identify which vaccinations you need? | 2.89 ± 0.03 | 2.92 ± 0.03 | 0.481 |
| 2. Can you understand your risk for mental health issues such as stress or depression? | 2.78 ± 0.03 | 2.85 ± 0.03 | 0.095 | |
| 3. Do you recognize signs of health problems caused by smoking, excessive drinking, or lack of exercise? | 2.85 ± 0.03 | 2.89 ± 0.03 | 0.360 | |
| 4. Can you identify which of your daily activities affect your health? | 2.90 ± 0.03 | 2.93 ± 0.03 | 0.466 | |
| 5. Can you understand your doctor’s explanations and instructions during treatment? | 3.07 ± 0.03 | 3.06 ± 0.03 | 0.691 | |
| 6. Do you know what to do first in an emergency? | 2.90 ± 0.03 | 2.87 ± 0.03 | 0.500 | |
| 7. Can you understand how to take medication when explained by a doctor or pharmacist? | 3.15 ± 0.02 | 3.18 ± 0.03 | 0.356 | |
| 8. Can you understand patient education materials provided by the hospital? | 2.93 ± 0.03 | 2.97 ± 0.03 | 0.350 | |
| 9. Can you judge whether health information from the Internet or media is trustworthy? | 2.73 ± 0.02 | 2.72 ± 0.03 | 0.674 | |
| 10. Can you use health information from the Internet or media to make health-related decisions? | 2.71 ± 0.03 | 2.72 ± 0.03 | 0.707 | |
| Total | 28.73 ± 0.24 | 28.97 ± 0.22 | 0.409 | |
*by complex sample chi-square test, †by complex sample linear regression analysis, p<0.05.
SD: standard deviation; GAD: generalized anxiety disorder group; Without_GAD: without generalized anxiety disorder group.
The findings regarding oral health problems in postmenopausal women, stratified by the presence or absence of GAD, are detailed in <Table 3>. The mean chewing difficulty score was significantly higher in the GAD group compared to those without GAD (p<0.05). While difficulties in speaking function were observed more frequently in the GAD group, this difference was not statistically significant.
Table 3. Differences in oral function problems according to generalized anxiety disorder in postmenopausal women (Unit: Mean±SD)
| Characteristics | Without_GAD (N=662) | GAD (N=535) | p* |
|---|---|---|---|
| Problems with chewing function | 2.20 ± 0.05 | 2.41 ± 0.05 | 0.003 |
| Problems with speaking function | 1.59 ± 0.04 | 1.67 ± 0.05 | 0.153 |
*by complex sample linear regression analysis.
SD: standard deviation; GAD: generalized anxiety disorder group; Without_GAD: without generalized anxiety disorder group.
The mediating role of health literacy in the relationship between GAD and impairments in chewing function among postmenopausal women is presented in <Table 4>, <Table 5>, and <Fig. 3>. After adjusting for sociodemographic factors and comorbid conditions, GAD, as the independent variable, demonstrated a statistically significant negative effect on health literacy, the mediator, with a regression coefficient (β) of −0.108 (p<0.01). In turn, health literacy exhibited a statistically significant negative association with chewing function impairments, the dependent variable, with a regression coefficient (β) of −0.015 (p<0.01). Additionally, the direct effect of GAD on chewing function impairments was positive and statistically significant, with a regression coefficient (β) of 0.051 (p<0.001).
The indirect effect of health literacy on the association between GAD and chewing function impairments was estimated at 0.002. The 95% bootstrap confidence interval for this indirect effect ranged from 0.001 (BootLLCI) to 0.004 (BootULCI), excluding zero, thereby indicating the statistical significance of the mediating effect. These results suggest that health literacy partially mediates the relationship between GAD and chewing function problems in postmenopausal women.
Table 4. The mediating effect of health literacy on the relationship between generalized anxiety disorder and chewing problem
| Variables | Health literacy | Problem with chewing function | ||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | t | p* | β | SE | t | p* | |
| Generalized anxiety disorder | -0.108 | 0.037 | -2.912 | 0.004 | 0.051 | 0.009 | 5.831 | <0.001 |
| Health literacy | -0.015 | 0.006 | -2.479 | 0.013 | ||||
| F(p) | 53.478(<0.001) | 14.887(<0.001) | ||||||
| R2 | 0.413 | 0.250 | ||||||
*by mediation effect analysis. SE: standard error. Adjusted for sociodemographic characteristics and comorbidities.
Table 5. Results of the significance test on the indirect effect of health literacy
| Variables | Effect | BootSE | 95% CI | |
|---|---|---|---|---|
| BootLLCI | BootULCI | |||
| Health literacy | 0.002 | 0.001 | 0.001 | 0.004 |
Bootstrap samples=5,000; SE: standard error; CI: confidence interval; LLCI: lower limit CI; ULCI: upper limit CI.
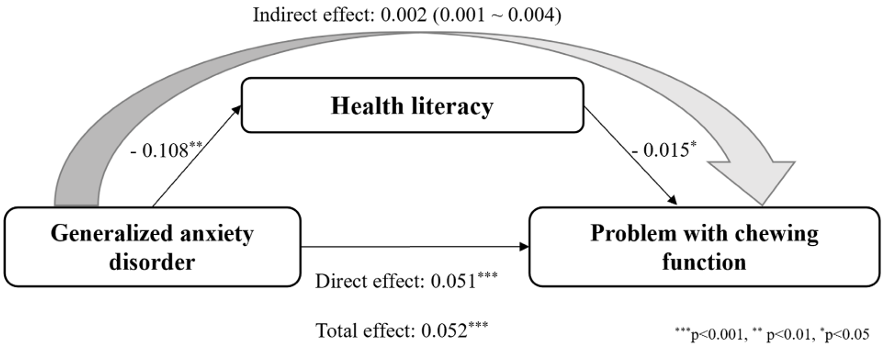
Fig. 3. The mediating effect of health literacy on the relationship between generalized anxiety disorder and chewing problem
<Table 6>, <Table 7>, and <Fig. 4> present the mediating role of health literacy in the relationship between GAD and speaking function impairments among postmenopausal women. After controlling for sociodemographic factors and comorbid conditions, GAD, as the independent variable, was found to have a statistically significant negative effect on health literacy, the mediator, with a regression coefficient (β) of −0.109 (p<0.01). In turn, health literacy exhibited a statistically significant negative association with speech function impairments, the dependent variable, with a regression coefficient (β) of −0.012 (p<0.05). Additionally, the direct effect of GAD on speech function impairments was positive and statistically significant, with a regression coefficient (β) of 0.035 (p<0.001).
In analyzing the relationship between the independent and dependent variables, the indirect effect mediated was estimated at 0.001. Since the 95% bootstrap confidence interval, ranging from 0.001 (BootLLCI) to 0.003 (BootULCI), does not include zero, this indirect effect is considered to represent a statistically significant mediating effect.
Table 6. The mediating effect of health literacy on the relationship between generalized anxiety disorder and speaking problem
| Variables | Health literacy | Problem with speaking function | ||||||
|---|---|---|---|---|---|---|---|---|
| β | SE | t | p* | β | tSE | t | p* | |
| Generalized anxiety disorder | -0.109 | 0.037 | -2.935 | 0.003 | 0.035 | 0.007 | 4.915 | <0.001 |
| Health literacy | -0.012 | 0.005 | -2.537 | 0.011 | ||||
| F(p) | 53.202(<0.001) | 16.108(<0.001) | ||||||
| R2 | 0.412 | 0.260 | ||||||
*by mediation effect analysis. SE: standard error. Adjusted for sociodemographic characteristics and comorbidities
Table 7. Results of the significance test on the indirect effect of health literacy
| Variables | Effect | BootSE | 95% CI | |
|---|---|---|---|---|
| BootLLCI | BootULCI | |||
| Health literacy | 0.001 | 0.001 | 0.001 | 0.003 |
Bootstrap samples= 5,000, SE: standard error; CI: confidence interval; LLCI: lower limit CI; ULCI: upper limit CI.
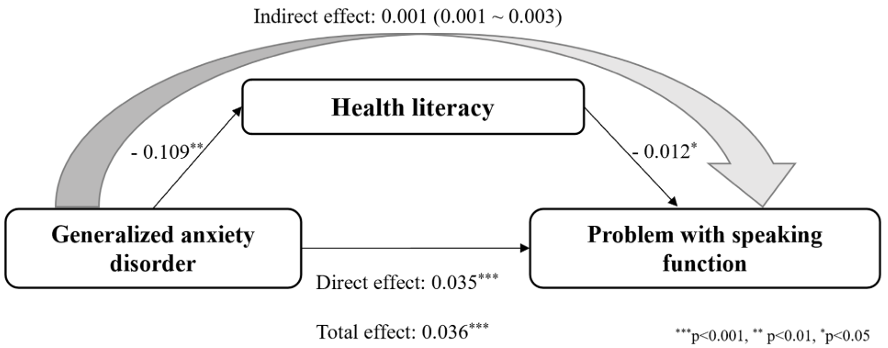
Fig. 4. The mediating effect of health literacy on the relationship between generalized anxiety disorder and speaking problem
This study utilized data from the 2023 KNHANES to examine the association between GAD and oral functional impairments, specifically difficulties in chewing and speaking, among Korean postmenopausal women. Furthermore, the research investigated the mediating role of health literacy in this relationship. The analysis revealed that individuals with GAD experienced significantly greater chewing difficulties compared to those without GAD. Additionally, GAD was found to significantly reduce health literacy, which in turn had a notable indirect effect in worsening both chewing and speaking impairments, thereby providing statistical evidence for the mediating role of health literacy. These findings align with previous studies linking mental health disorders to oral health outcomes [6,8,9], and this study uniquely contributes by empirically validating this association within the specific population of postmenopausal women.
Postmenopausal women represent a demographic characterized by heightened susceptibility to both GAD and oral functional impairments, attributable to a combination of biological and psychosocial factors. The reduction in estrogen levels during menopause is linked to decreased salivary secretion, mucosal atrophy, xerostomia, and increased vulnerability of periodontal tissues, collectively exacerbating oral functional decline [2]. Psychological stressors, including anxiety, further activate the sympathetic nervous system and contribute to harmful oral behaviors such as bruxism and temporomandibular joint strain, which may intensify pain and impair masticatory performance [3,4,9,11]. Additionally, postmenopausal women often experience concomitant conditions such as alveolar bone resorption, reduced bone mineral density, and age-related deterioration of masticatory function, rendering them more functionally vulnerable compared to other demographic groups defined by age and gender. Unlike previous studies that primarily focused on young adults or the general adult population, the present study is distinguished by its emphasis on postmenopausal women, a cohort undergoing intersecting physiological and psychological changes. A key finding of this study is the significant mediating role of health literacy in the relationship between GAD and oral functional impairments. Health literacy involves not only the acquisition of health-related information but also the ability to comprehend, critically evaluate, and apply such information to promote effective health behaviors [13]. Individuals with elevated anxiety levels frequently experience deficits in attention, cognitive processing, and problem-solving skills, which hinder their ability to assimilate complex health information and implement appropriate behavioral strategies. The results of this study suggest an indirect pathway whereby reduced health literacy impairs the adoption of oral health management practices, ultimately leading to functional decline. Empirical evidence supports that populations with low health literacy are less likely to engage in preventive oral health behaviors—such as interdental cleaning, use of oral rinses, and fluoride application—and are more likely to delay dental consultations when early symptoms arise [14]. These findings highlight that improving health literacy extends beyond increasing knowledge; it represents a crucial mediating mechanism for restoring self-efficacy diminished by anxiety and promoting preventive oral health behaviors.
Although the indirect effects identified in this study (0.002 for chewing function impairments and 0.001 for speaking function impairments) are statistically significant, the absolute effect sizes are relatively small. However, these findings should be understood not as substantial changes at the individual level but as clinically and practically meaningful indicators at the population level. This implies that even slight enhancements in health literacy among postmenopausal women with GAD may reduce the cumulative risk of oral functional decline within this population.
Among postmenopausal women—who face an elevated risk of progressive tooth loss, denture dependency, masticatory dysfunction, and subsequent social withdrawal—the early identification of high-risk subpopulations characterized by coexisting mental health conditions, such as GAD, and limited health literacy is essential. The implementation of targeted educational interventions, counseling, and comprehensive oral health management for these groups may constitute a clinically significant preventive strategy.
Oral functional decline encompasses more than simple discomfort; it significantly impairs the oral health-related quality of life (OHRQoL) in postmenopausal women. Previous studies have established that functional oral health problems, such as difficulties with mastication and speech, are closely associated with diminished OHRQoL due to challenges in eating, articulation, and social interaction [19–21]. Importantly, in elderly and vulnerable populations, masticatory impairments have been correlated with limited nutritional intake and declining overall health, whereas speech difficulties may lead to social isolation and psychological withdrawal.
The pathway elucidated in this study—where GAD influences health literacy, subsequently impacting oral functional impairments—carries important clinical implications. This sequence indicates not only an immediate decline in oral function but also a heightened risk of progressive deterioration in OHRQoL over the medium to long term.
These results carry substantial implications for both clinical practice and public health initiatives. Primarily, oral health care for postmenopausal women should not be limited to routine dental examinations and educational activities; rather, it should encompass systematic screening for anxiety and the provision of individualized interventions. The integration of brief screening instruments, such as the GAD 7-item scale, within primary care and dental environments can effectively identify individuals at heightened risk for GAD. Following identification, appropriate referrals to mental health services or the establishment of multidisciplinary collaboration frameworks involving dental, mental health, and women’s health specialists are both practicable and beneficial from a clinical perspective. Furthermore, efforts to improve health literacy must go beyond the simple transmission of information and actively promote the conversion of knowledge into practical health behaviors. This objective may be accomplished through cognitive-behavioral strategies, including the use of clear, accessible language tailored to the patient’s level of understanding, the incorporation of visual supports, experiential learning methods, and structured behavioral planning [13–15].
Specifically, for individuals presenting with heightened anxiety, tailored educational approaches that address the quality of information, modes of delivery, and practical relevance are essential. This suggests that improving health literacy could serve as a viable intervention to reduce indirect functional deterioration linked to anxiety. In particular, for postmenopausal women who may experience an increased cognitive load as a result of elevated anxiety, it is clinically important to provide oral health education through succinct and focused messaging, repeated instructional sessions, and the engagement of family members.
Thirdly, the implementation of programs that combine mental health education with oral health education targeting high-risk populations—specifically individuals with GAD or socioeconomically vulnerable postmenopausal women—within communitybased interventions, such as those delivered at public health centers and local dental health facilities, is highly feasible. Such integrated approaches have the potential to promote more favorable dental care utilization patterns and to enhance OHRQoL in the long term.
This study is significant in that it empirically elucidates the mediating mechanisms linking GAD, health literacy, and oral health functional impairments among postmenopausal women, drawing upon large-scale data representative of the national population. Nonetheless, given its cross-sectional design, the study precludes causal interpretations. Furthermore, the exclusive use of selfreported measures for both health literacy and oral functional difficulties raises concerns regarding potential response bias. Importantly, unlike knowledge-based health literacy items that assess accuracy of responses, none of the ten self-reported items exhibited significant differences between GAD groups, suggesting that these measures should be applied with caution. Moreover, although the health literacy metric employed in the KNHANES [15] offers a broad overview, it lacks the granularity necessary for in-depth analysis of specific dimensions such as comprehension, evaluation, and application. Furthermore, the relatively modest absolute magnitude of the indirect effect identified in this study suggests the existence of a mediating effect; nevertheless, it also indicates that the immediate clinical implications may be limited. This constraint should be taken into careful consideration when interpreting the results. Future investigations are encouraged to utilize oral health issues as mediating variables to facilitate comparative analyses. Moreover, the application of hierarchical regression analysis is recommended to more accurately quantify the extent of the mediating effect. Longitudinal research designs are also essential to clarify the temporal and causal relationships among GAD, health literacy, and oral functional impairments. Lastly, intervention studies evaluating the efficacy of programs aimed at improving health literacy in relation to actual functional outcomes and OHRQoL are warranted.
This study utilized data from the 2023 KNHANES to examine the mediating effect of health literacy on the relationship between GAD and oral health problems in Korean postmenopausal women.
1. An investigation into oral health problems among postmenopausal women demonstrated that individuals diagnosed with GAD experienced significantly more pronounced impairments in chewing function relative to their counterparts without GAD (p<0.05). While impairments in speaking function were observed more frequently within the GAD cohort, this difference did not achieve statistical significance.
2. The mediating role of health literacy in the relationship between GAD and chewing function impairments among postmenopausal women persisted as statistically significant, exhibiting an indirect effect of 0.002 (bootstrapped 95% confidence interval: 0.001 to 0.004), after adjusting for sociodemographic variables and comorbid conditions.
3. In the relationship between GAD and impairments in speaking function among postmenopausal women, health literacy demonstrated a statistically significant mediating effect. This indirect effect was quantified at 0.001, remaining significant after adjustment for sociodemographic factors and comorbid conditions (bootstrapped 95% confidence interval: 0.001 to 0.003).
These results indicate that menopause-associated GAD is associated with reduced oral health problems, with health literacy potentially serving as a mediating variable that mitigates these negative outcomes. Therefore, the design and implementation of oral health education interventions aimed at enhancing health literacy, alongside strategies for anxiety management, are recommended.
Conceptualization: YR Kim; Data collection: YR Kim; Formal analysis: YR Kim; Writing-original draft: YR Kim, DJ Kim, JY Lee; Writing-review&editing: YR Kim, DJ Kim, JY Lee
The authors declared no conflicts of interest.
None.
None.
The data used in this study are available from the Korea National Health and Nutrition Examination Survey (KNHANES) through the official access procedure of the Korea Disease Control and Prevention Agency.
None.
1. Freeman EW, Sammel MD, Lin H, Nelson DB. Associations of hormones and menopausal status with depressed mood in women with no history of depression. Arch Gen Psychiatry 2006;63(4):375–82. https://doi.org/10.1001/archpsyc.63.4.375