
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Mu-Yeol Cho1![]() , Je-Hyun Eom1
, Je-Hyun Eom1![]() , Ji-Won Kim1
, Ji-Won Kim1![]() , Yun-Woo Kim1
, Yun-Woo Kim1![]() , Seung-Jo Yang2
, Seung-Jo Yang2![]() , Jeong-Hoo Lee2
, Jeong-Hoo Lee2![]() , Hye-Sung Kim3
, Hye-Sung Kim3![]() , Jinhyeuk Lee4
, Jinhyeuk Lee4![]() , Inseong Hwang1
, Inseong Hwang1![]() , Young Youn Kim3
, Young Youn Kim3![]()
1Apple Tree Institute of Biomedical Science, Apple Tree Medical Foundation
2Docsmedi Co., Ltd.
3Apple Tree Dental Hospital, Apple Tree Medical Foundation
4Daesang Wellife Co., Ltd.
Correspondence to Young Youn Kim, Apple Tree Dental Hospital, Apple Tree Medical Foundation, 1450, Jungang-ro, Ilsanseo-gu, Goyangsi, Gyeonggi-do, 10387, Republic of Korea. Tel: +82-70-4601-5479, E-mail: rladuddus@appleden.com
Volume 26, Number 3, Pages 307–18, June 2026.
J Korean Soc Dent Hyg 2026;26(3):307–18. https://doi.org/10.13065/jksdh.2026.26.3.4
Received on January 21, 2026, Revised on May 22, 2026, Accepted on June 05, 2026, Published on June 30, 2026.
Copyright © 2026 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Gingivitis, Probiotics, Randomized clinical trial, Root planing, Scaling
Periodontal tissues are key components of oral health that support and protect teeth, and chronic inflammation of these periodontal tissues causes periodontal disease, which is a major cause of tooth loss [1]. To prevent and treat periodontal disease, it is essential to eliminate the causes of oral inflammation, with biofilm being the most widely recognized risk factor [2]. Scaling and root planing (SRP) is an essential method in periodontal treatment for removing bacterial biofilm and calculus [3]. However, considering the anatomical and instrumental limitations of such mechanical treatment, complete removal of all bacterial biofilm is unrealistic [4]. Adjunctive therapies such as antibiotics and probiotics have been proposed to enhance the effectiveness of SRP [5,6]. While there are clear clinical benefits when antibiotics are used as adjunctive therapy in periodontal treatment, concerns have been raised about side effects such as vomiting, diarrhea, and allergies, as well as public health concerns about antibiotic resistance [7,8].
Probiotics, which are living microorganisms, are receiving worldwide attention as an alternative biological approach [9]. Previous studies have reported that clinical improvement in periodontitis was observed when probiotics were taken in conjunction with mechanical treatment, showing results similar to antibiotics [10]. A meta-analysis of 21 clinical studies applying probiotics as adjunctive therapy in periodontal treatment showed significant improvement in probing depth (PD), clinical attachment level, and bleeding on probing (BOP) compared to the control group [11]. Taking probiotics has fewer side effects and can prevent side effects such as antibiotic-associated diarrhea [12]. However, the types and combinations of probiotics used in various studies, as well as their forms of administration and application methods, differ. Therefore, well-designed new studies are needed to evaluate the effects of newly discovered probiotics on periodontal tissues.
Lactobacillus is a major probiotic strain known to be effective for oral health [13]. Lactobacillus plantarum DSR920 is a probiotic isolated from cabbage kimchi that has been reported to alter the intestinal microbial community, enhance regulatory T cell immunity, suppress inflammatory responses, and prevent and improve obesity [14]. Lacticaseibacillus rhamnosus DM163, another type of probiotic, has been reported to have halitosis suppression and antimicrobial properties when products containing this bacterial strain are consumed [15]. Considering that L. plantarum DSR920 primarily exerts immunomodulatory effects through regulatory T cell enhancement, while L. rhamnosus DM163 exhibits direct antimicrobial activity against oral pathogens, the combination of these two strains may provide synergistic benefits for periodontal health through dual mechanisms of action. However, there have been no studies evaluating the combined consumption of these two strains to date.
Therefore, the objective of this study was to evaluate the adjunctive effects of combined L. rhamnosus DM163 and L. plantarum DSR920 probiotics following SRP on gingival inflammation, inflammatory biomarkers, oral microbiota, and safety in patients with mild gingivitis.
This study protocol was described based on the SPIRIT guidelines [16], and was conducted in compliance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Board of Apple Tree Medical Foundation (IRB No.\ATDH-2023-0002; approval date: March 16, 2023). Written informed consent was obtained from all participants prior to enrollment. The trial was retrospectively registered with the Clinical Research Information Service of the National Research Institute of Health in the Republic of Korea (KCT0009762) on September 6, 2024, after data collection had been completed. The study protocol, including outcomes, eligibility criteria, intervention, and analysis plan, was prospectively defined and approved by the IRB (ATDH-2023-0002; March 16, 2023) before the enrollment of the first participant.
This study was a single-center, double-blind, parallel-group, stratified randomized pilot clinical trial. The trial was conducted at Apple Tree Dental Hospital located in Goyang-si, Republic of Korea, from March 2023 to August 2024. The study procedures progressed in the following order: Visit 1 (consent and examination, SRP), Visit 2 (randomization and baseline) 4 weeks after Visit 1. This 4-week interval was designed to allow adequate time for initial tissue healing and stabilization following SRP, ensuring that baseline measurements reflected a post-healing state rather than acute inflammatory responses [4,17]. At Visit 1, a series of interviews and clinical examinations were performed to assess participant eligibility. Clinical examinations included PD, gingival index (GI), plaque index (PI), BOP, gingival recession (GR), and CAL (clinical attachment level). Additionally, dental radiographic examination, SRP, and safety tests were performed. Visit 2 was the baseline of the study, the point at which participants began consuming the probiotic combination or placebo. Clinical and microbiological evaluations were repeated at Visit 2 and subsequent Visits 3 and 4. In particular, at Visit 4, additional dental radiographic and safety tests were performed. The primary outcomes were PD and GI. Secondary outcomes included oral bacterial counts and other clinical parameters (BOP, PI, GR, CAL). The number of subjects in this study was calculated to be 15 per group, 30 in total, based on previous studies [18].
Mild gingivitis was defined according to the 2018 American Academy of Periodontology and European Federation of Periodontology classification of periodontal and peri-implant diseases and conditions, which uses a bleeding on probing (BOP) score of ‾10% as the principal diagnostic criterion for gingivitis on an intact periodontium [19]. Participant selection criteria included adults between 19 and 70 years of age, those who had at least one Ramfjord tooth with PD between 3 mm and 5 mm at six sites, those who had BOP at 10% or more of Ramfjord tooth sites, and those who had 20 or more natural teeth.
Exclusion criteria included oral health status and systemic health status. Those who had received scaling within the last month, those who had received periodontal treatment within the last 6 months, those with serious pathological findings in oral soft tissue, those requiring immediate caries treatment or surgery or acute treatment of periodontitis, and those with moderate periodontitis symptoms who were currently receiving drug treatment or required medication were excluded. Regarding systemic health, those with clinically significant cardiovascular, immunological, infectious, or neoplastic diseases, those with uncontrolled hypertension (160/100 mmHg or higher after 10 minutes of rest) and uncontrolled diabetes patients (fasting blood glucose level of 180 mg/dL or higher or initiation of diabetes medication within the last 3 months), those with mental illness such as schizophrenia, depression, drug addiction, or alcoholism, those with a history of bleeding disorders, and those taking antiplatelet or anticoagulant agents were excluded. Those diagnosed with cancer within the last 5 years were also excluded. Additionally, those who had taken medications affecting periodontal status (phenytoin, calcium channel blockers, cyclosporine, coumadin, non-steroidal anti-inflammatory drugs, aspirin, etc.) for 5 consecutive days or more during the last month, those who had used antibiotics or adjunctive periodontal disease treatment within the last month, and women who were planning pregnancy or lactation during the study participation period or within 6 months postpartum were excluded.
The random allocation sequence was generated by an independent statistician using stratified block randomization in R (version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria), with age (in 10-year units) and sex as stratification factors. Allocation numbers were written in sealed envelopes to assign subjects to the test group or placebo group. Participants were enrolled by M.Y.C., who had no access to the allocation sequence until group assignment. Double-blinding was applied to both investigators and subjects, and information was disclosed only to the principal investigator and statistical analyst in case of dropout or adverse events. The test product was a powder mixture of L. plantarum DSR920 and L. rhamnosus DM163 in a 3:1 ratio and was manufactured together with the placebo by VITECH Inc.<Table 1>. The probiotic and placebo were designed to have the same taste and form and included inactive ingredients such as fructooligosaccharides and sweeteners for consistency. The daily intake amount and method was to consume one packet (2 g, total viable count 100 billion colony-forming units) once a day, after dinner or before sleep after oral hygiene care, dissolved in approximately 50 mL of water, and not to perform oral hygiene immediately after consumption. The intake period was set at 12 weeks from the study baseline.
Table 1. Composition of probiotic prototype and placebo
| Ingredients | L. plantarum DSR920 | L. rhamnosus DM163 | Maltodextrin | Organic rice flour | Enzyme-treated stevia | Silicon dioxide | Mixed grain powder flavor |
|---|---|---|---|---|---|---|---|
| Probiotics | 9.7 (7.5E10 CFU) | 5.5 (2.5E10 CFU) | 74.8 | 7 | 1.5 | 1 | 0.5 |
| Placebo | 0 | 0 | 89 | 8 | 1.5 | 1 | 0.5 |
Values are expressed as percentage (%) of total weight. CFU, colony-forming unit.
Major periodontal indicators such as PD, GI, PI, BOP, GR, and CAL were performed as clinical measurement items. Clinical measurements were performed on Ramfjord teeth (maxillary right first molar, maxillary left central incisor, maxillary left first premolar, mandibular left first molar, mandibular right central incisor, mandibular right first premolar) [20]. Measurements were taken at six sites of each Ramfjord tooth (mesiobuccal, midbuccal, distobuccal, mesiolingual, midlingual, distolingual). Two trained dental professionals underwent training before the trial to ensure consistency and reliability, achieving a Kappa result of 0.92 in inter-examiner reliability assessment. A North Carolina periodontal probe (Hu-Friedy, Chicago, IL, USA) was used to measure PD and GR. GI was scored using the Löe and Silness gingival index (0-3) [21], and PI was scored using the Silness and Löe plaque index (0-3) [21]. BOP was calculated as the percentage of sites exhibiting bleeding on probing among all examined sites [(number of bleeding sites / total examined sites) × 100]. CAL was calculated as the sum of PD and GR. These examinations were performed at each patient visit during the study period. Additionally, panoramic X-ray examination was performed during the screening phase and at the final visit. During the screening process, radiographs were used to assess the structural status of teeth and periodontal tissues, confirm the number of natural teeth, and evaluate the feasibility of Ramfjord tooth examination. X-ray examination at the final visit was used to observe overall oral status changes during the study period and evaluate treatment outcomes.
Oral microbial analysis was performed using quantitative real-time polymerase chain reaction (qPCR). Sample collection was conducted on supragingival plaque (biofilm) and mouthwash samples. Plaque samples were collected from Ramfjord teeth using Gracey curettes (11/12, 13/14, Hu-Friedy, Chicago, IL, USA) and stored in phosphate-buffered saline (pH 7.0). Mouthwash sample collection used the Oralbiome CHECK kit (Docsmedi Co., Ltd., Korea), which included mouthwash solution and dedicated tubes. Participants rinsed vigorously for 30 seconds with the provided solution and then spat it into the collection tube. Genomic DNA was extracted from samples using the Bacteria Genomic DNA Isolation Kit (LaboPass, COSMO genetech, Korea) according to the manufacturer’s instructions. Six microorganisms were quantitatively analyzed in each sample. Periodontal pathogens included three species of the red complex (Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola) and three species of the orange complex (Prevotella intermedia, Campylobacter rectus, Fusobacterium nucleatum). Bacterial counts were log10-transformed for analysis and are reported as log10 DNA copy number.
Safety evaluation was performed using the safety set, which included all participants who were randomized and consumed the study product at least once. Blood pressure and hematological and chemical analyses were performed to evaluate adverse events. For accurate measurement, participants were instructed to maintain fasting for 8 hours before the visit. After blood collection, blood samples were immediately centrifuged using a centrifuge (DM0408, DLAB Scientific Co.\LTD., China). Separated serum samples were analyzed in blood chemistry tests using the BioSystems A25 analyzer (Spain). Blood tests included WBC, RBC, Hb, Hct, Platelet, ALT (GPT), BUN, and C-reactive protein.
Serum inflammatory biomarkers (IL-1β, IL-6, TNF-α) were measured using ELISA and are provided in <Supplementary Table S3>.
The data collected in this study were classified into safety set, full analysis set (FA set), and per-protocol set (PP set). The safety set included all participants who consumed the test product at least once. Based on the intention-to-treat principle, the FA set included all participants who consumed the test product at least once, participated in efficacy evaluation at 6 and 12 weeks, and met inclusion/exclusion criteria. The PP set included only participants who completed this study while complying with all protocol requirements. The FA set was primarily used for efficacy evaluation to maximize statistical power in this pilot study, and PP set analysis was additionally performed as a sensitivity analysis. The safety set was used only for safety analysis.
Statistical analyses were performed using R (version 4.4.1; R Foundation for Statistical Computing, Vienna, Austria). Data were presented as median (interquartile range, IQR) for continuous variables and n (%) for categorical variables. Between-group comparisons were analyzed using the Mann-Whitney U test for continuous variables and Fisher’s exact test for categorical variables. Within-group changes across the three time points were assessed using the Friedman test, with post-hoc pairwise comparisons performed using the Wilcoxon signed-rank test with Bonferroni correction. The FA set was used as the primary analysis population, with PP set results provided as supplementary material. Missing data were not imputed. The significance level (α) was set at 0.05.
Participants were instructed to maintain their usual oral hygiene practices. No additional periodontal treatments were provided during the study period.
A total of 30 participants were enrolled and randomized. Three participants withdrew before completing any post-baseline assessment and were excluded from analysis. The FA set included 27 participants (test: n=14, placebo: n=13) who completed at least one post-baseline assessment. The PP set included 18 participants (test: n=8, placebo: n=10) who completed the study without protocol violations <Fig. 1>. Given the small sample size of this pilot study, the FA set was used for primary analysis to maximize statistical power. PP set results are provided in <Supplementary Tables S1-S2>.
Baseline characteristics were similar between groups <Table 2>. Median age was 43 years in the test group and 47 years in the placebo group (p=0.593). No significant differences were observed in sex distribution, lifestyle factors, or anthropometric measurements.
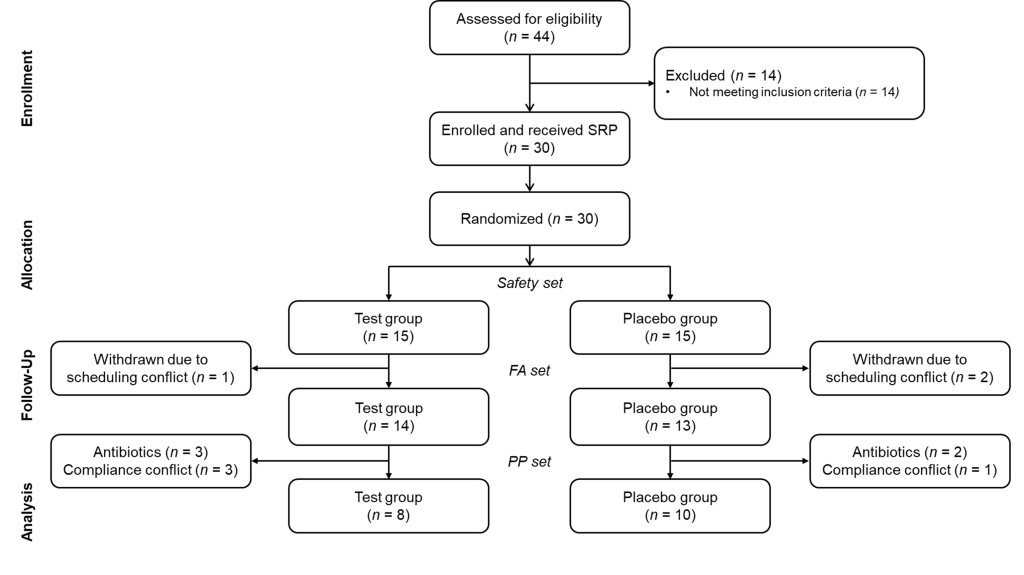
Fig. 1. Flowchart depicting the study design. FA, full analysis; PP, per protocol.
Table 2. Demographics and clinical characteristics of baseline
| Variables | Test (n=14) | Placebo (n=13) | p-value |
|---|---|---|---|
| Age | 43.00 (30.75-55.75) | 47.00 (33.00-54.00) | 0.593 |
| Sex | 1.000 | ||
| Male | 6 (42.9) | 6 (46.2) | |
| Female | 8 (57.1) | 7 (53.8) | |
| Smoking status | 1.000 | ||
| Smoker | 5 (35.7) | 5 (38.5) | |
| Non-smoker | 9 (64.3) | 8 (61.5) | |
| Drinking status | 0.596 | ||
| Drinker | 11 (78.6) | 12 (92.3) | |
| Non-drinker | 3 (21.4) | 1 (7.7) | |
| Sleep duration | 0.789 | ||
| 8-10 hours | 2 (14.3) | 1 (7.7) | |
| 6-8 hours | 7 (50.0) | 8 (61.5) | |
| 4-6 hours | 5 (35.7) | 4 (30.8) | |
| Brushing duration | 0.397 | ||
| ≥3 min | 0 (0.0) | 1 (7.7) | |
| 2-3 min | 5 (35.7) | 5 (38.5) | |
| 1-2 min | 7 (50.0) | 7 (53.8) | |
| <1 min | 2 (14.3) | 0 (0.0) | |
| Floss use frequency | 0.501 | ||
| Daily | 1 (7.1) | 0 (0.0) | |
| 5 times/week | 1 (7.1) | 0 (0.0) | |
| 3 times/week | 1 (7.1) | 2 (15.4) | |
| 1 time/week | 1 (7.1) | 0 (0.0) | |
| Never | 10 (71.4) | 11 (84.6) | |
| Interdental cleaning frequency | 0.437 | ||
| Daily | 1 (7.1) | 2 (15.4) | |
| 5 times/week | 1 (7.1) | 0 (0.0) | |
| 3 times/week | 0 (0.0) | 2 (15.4) | |
| 1 time/week | 1 (7.1) | 1 (7.7) | |
| Never | 11 (78.6) | 8 (61.5) | |
| Weight (kg) | 66.50 (60.25-76.75) | 58.00 (54.00-72.00) | 0.466 |
| Height (cm) | 163.50 (161.00-173.00) | 168.00 (155.00-176.00) | 1.000 |
| BMI (kg/m2) | 25.00 (23.25-26.00) | 23.00 (21.00-26.00) | 0.380 |
| Systolic BP (mmHg) | 127.50 (123.25-137.25) | 132.00 (123.00-136.00) | 0.981 |
| Diastolic BP (mmHg) | 79.50 (71.75-85.25) | 83.00 (74.00-89.00) | 0.466 |
Data are presented as median (IQR) for continuous variables and n (%) for categorical variables. BMI, body mass index; BP, blood pressure; IQR, interquartile range. p-values were calculated using the Mann-Whitney U test for continuous variables and Fisher’s exact test for categorical variables.
Clinical periodontal parameters at baseline, 6 weeks, and 12 weeks are summarized in <Table 3>. No statistically significant changes were observed in either group across the three time points for any clinical parameter, including GI, BOP, PD, GR, PI, and CAL (Friedman test, all p>0.05). Between-group comparisons at each time point also showed no significant differences (Mann-Whitney U test, all p>0.05).
Table 3. Changes in clinical periodontal parameters over 12 weeks
| Clinical Parameters | Time Point | Test (n=14) | Placebo (n=13) | p-valueb |
|---|---|---|---|---|
| GI | Baseline | 0.69 (0.44-0.97) | 0.58 (0.25-0.83) | 0.497 |
| 6 weeks | 0.54 (0.22-0.68) | 0.53 (0.39-0.81) | 0.627 | |
| 12 weeks | 0.44 (0.22-0.71) | 0.39 (0.22-0.50) | 0.542 | |
| p-valuea | 0.451 | 0.375 | ||
| BOP (%) | Baseline | 19.4 (13.2-29.2) | 16.7 (11.1-22.2) | 0.393 |
| 6 weeks | 16.7 (9.7-23.6) | 22.2 (11.1-27.8) | 0.393 | |
| 12 weeks | 19.4 (9.0-24.3) | 13.9 (8.3-22.2) | 0.494 | |
| p-valuea | 0.590 | 0.734 | ||
| PD (mm) | Baseline | 2.13 (1.95-2.25) | 2.11 (2.00-2.22) | 0.752 |
| 6 weeks | 2.08 (1.83-2.22) | 2.14 (2.00-2.33) | 0.560 | |
| 12 weeks | 1.93 (1.87-2.32) | 2.17 (1.94-2.42) | 0.296 | |
| p-valuea | 0.872 | 0.376 | ||
| GR (mm) | Baseline | 0.15 (0.00-0.26) | 0.00 (0.00-0.14) | 0.431 |
| 6 weeks | 0.13 (0.01-0.24) | 0.08 (0.00-0.17) | 0.533 | |
| 12 weeks | 0.19 (0.06-0.31) | 0.06 (0.00-0.31) | 0.447 | |
| p-valuea | 0.494 | 0.733 | ||
| PI | Baseline | 0.88 (0.69-1.03) | 0.81 (0.75-0.94) | 1.000 |
| 6 weeks | 0.88 (0.69-1.07) | 0.89 (0.72-1.03) | 0.923 | |
| 12 weeks | 0.96 (0.84-1.06) | 0.89 (0.78-1.06) | 0.662 | |
| p-valuea | 0.404 | 0.584 | ||
| CAL (mm) | Baseline | 2.22 (2.09-2.54) | 2.11 (2.00-2.75) | 0.846 |
| 6 weeks | 2.19 (2.03-2.42) | 2.28 (2.03-2.67) | 0.576 | |
| 12 weeks | 2.10 (2.00-2.55) | 2.28 (1.94-2.78) | 0.770 | |
| p-valuea | 0.444 | 0.451 |
Data are presented as median (IQR). GI, gingival index; BOP, bleeding on probing; PD, probing depth; GR, gingival recession; PI, plaque index; CAL, clinical attachment level; IQR, interquartile range. a Friedman test for overall changes across the three time points within each group. b Mann-Whitney U test for between-group comparison at each time point.
Changes in oral microbiota in mouthwash and plaque samples are presented in <Fig. 2>. In mouthwash samples, T. denticola showed a statistically significant increase in the placebo group at 6 weeks compared to baseline (Friedman p=0.010; post-hoc Bonferroni-adjusted p=0.005), while no significant change was observed in the test group. In plaque samples, F. nucleatum showed a statistically significant increase in the test group at 12 weeks compared to baseline (Friedman p=0.046; post-hoc Bonferroni-adjusted p=0.009). For the remaining species (P. gingivalis, T. forsythia, P. intermedia, and C. rectus), no statistically significant within-group changes were observed in either sample type.
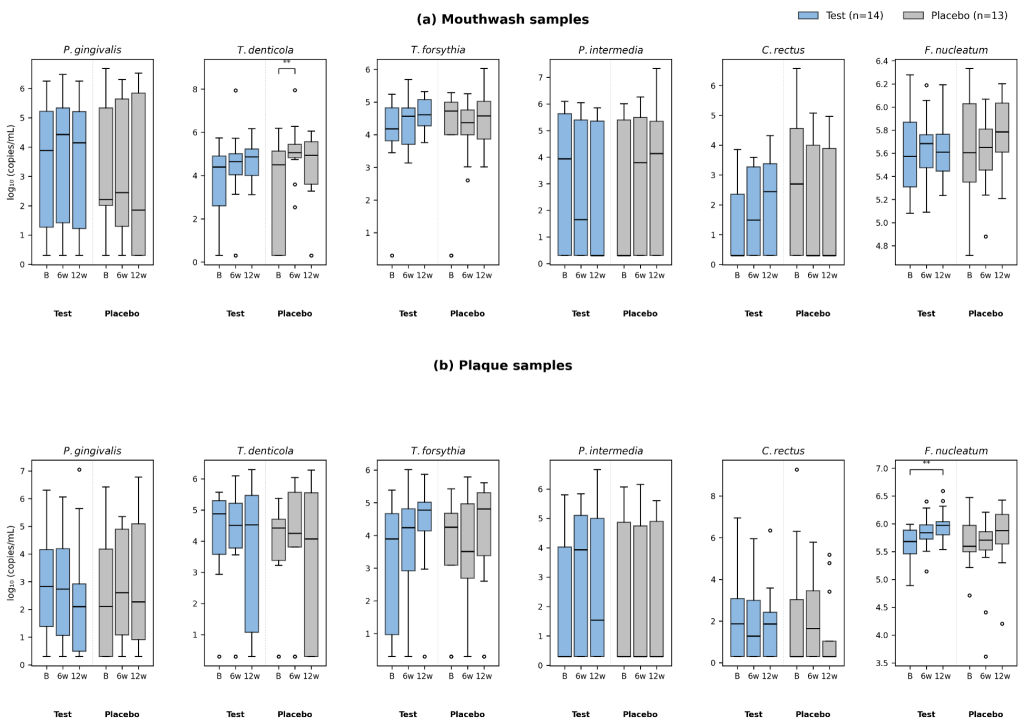
Fig. 2. Box plots of microbial counts (log10 copies/mL) at baseline, 6 weeks, and 12 weeks. (a) Mouthwash samples; (b) Plaque samples. Boxes represent the interquartile range, horizontal lines indicate medians, whiskers extend to 1.5× IQR, and circles denote outliers. Significance markers (**, p<0.01) indicate Bonferroni-adjusted Wilcoxon signed-rank post-hoc comparisons following a significant Friedman test (p<0.05) for within-group changes across the three time points.
No serious adverse events occurred. Clinical pathology tests, vital signs, and anthropometric measurements showed no significant changes after 12 weeks. Serum inflammatory biomarkers were mostly below detection limits or at low levels <Supplementary Table S3>.
This randomized, double-blind pilot clinical trial evaluated the adjunctive effects of 12-week supplementation with a combined probiotic formulation (L. rhamnosus DM163 and L. plantarum DSR920) following SRP on periodontal health in patients with mild gingivitis. No statistically significant between-group superiority or consistent beneficial changes were observed in clinical periodontal parameters or in the major periodontal pathogens. The product was well tolerated throughout the 12-week intervention period, with no serious adverse events. Therefore, the findings should not be interpreted as definitive evidence that the probiotic combination has no biological or clinical potential, but rather as indicating that no additional adjunctive benefit was detected under the present post-SRP, mild-gingivitis study conditions.
The absence of significant changes in clinical parameters should be interpreted in the context of several methodological considerations. As participants were patients with mild gingivitis who had received SRP four weeks before baseline, their clinical indices were already close to the normal range at the time of randomization, suggesting a floor effect in which the potential for detecting further improvement was substantially limited. A previous randomized clinical trial evaluating an oral health functional ingredient in patients with gingivitis and incipient periodontitis without prior scaling reported a similar pattern, in which intergroup differences in clinical parameters did not reach statistical significance despite favorable trends in both groups [22]. This convergent observation suggests that detecting adjunctive efficacy on clinical indices alone may be inherently difficult in mild gingivitis populations. Future trials may need to optimize baseline standardization, for example by carefully defining the interval between SRP and randomization or by evaluating the probiotic intervention in designs without prior SRP, depending on the intended clinical indication. The small sample size of the present pilot study also limited statistical power, and the possibility of type II error cannot be excluded.
In the microbiological analysis, two statistically significant within-group changes were identified: an increase in T. denticola in the placebo group (mouthwash, 6 weeks) and an increase in F. nucleatum in the test group (plaque, 12 weeks). Both changes represented increases from baseline rather than decreases, and the corresponding increase was not observed in the alternate group for each finding – T. denticola did not increase in the test group, and F. nucleatum did not increase in the placebo group. These group-specific patterns may reflect differences in microbial recolonization dynamics after SRP; however, they should not be interpreted as evidence of a clear antimicrobial effect of the probiotic combination. F. nucleatum is frequently detected in the oral cavity and functions as a bridging organism during oral biofilm maturation [23], and its increase observed at a single time point in a single sample type warrants careful interpretation. Given the exploratory nature of the microbiological analyses, both false-positive findings due to multiple comparisons and false-negative findings due to limited power and conservative correction should be considered.
Most serum inflammatory biomarkers were below detection limits in the present study. Detectable IL-1β was observed in only 8 of 27 cases in the FA set, consistent with the limited systemic inflammatory response associated with mild gingivitis. A previous immunological comparison reported no significant differences in serum IL-1β and TNF-α between subjects with and without periodontal disease [24]. In contrast, the same biomarkers measured in gingival crevicular fluid (GCF) have shown clear differences between groups in clinical trials evaluating oral health functional ingredients in gingivitis patients, with significant reductions in IL-1β, PGE2, MMP-8, and MMP-9 reported after eight weeks of supplementation [22]. These observations support the use of GCF-based biomarker assessment as a more sensitive measurement strategy in future trials.
This study has several limitations. First, the sample size was small, and the number of participants excluded from the PP set because of dropout or protocol deviations was relatively high. Second, because all participants received SRP before randomization, baseline clinical parameters reflected a post-therapeutic, near-healthy condition, limiting the ability to detect additional probiotic benefits (floor effect). Third, the FA set excluded early dropouts and therefore does not constitute a true intention-to-treat analysis; missing data were not imputed. Fourth, clinical assessments were limited to six Ramfjord teeth, which may reduce sensitivity compared to full-mouth examination, and future studies should consider site-level or multi-tooth analyses. Fifth, most serum inflammatory biomarkers were below detection limits, suggesting that GCF-based measurement may be more appropriate for detecting local inflammatory responses in mild gingivitis. Finally, because microbiological outcomes were assessed across multiple species, sample types, and time points, the findings should be interpreted as exploratory. Despite these limitations, this study provides initial safety data and methodological insights that can inform the design of larger-scale confirmatory trials of this probiotic combination, particularly in patients with more pronounced gingival inflammation.
This randomized, double-blind pilot clinical trial is the first to evaluate the adjunctive effects of combined Lacticaseibacillus rhamnosus DM163 and Lactobacillus plantarum DSR920 following SRP in patients with mild gingivitis, and the findings indicate that more refined trial designs are needed to identify clinically meaningful applications. The study included 27 participants in the analysis (Test, n=14; Placebo, n=13), and the following conclusions were drawn:
1. Under the present post-SRP mild-gingivitis study conditions, 12-week adjunctive supplementation with the combined probiotic did not result in statistically significant additional improvements in clinical periodontal parameters (GI, BOP, PD, GR, PI, and CAL) compared with placebo.
2. No consistent reductions in major periodontal pathogens (P. gingivalis, T. forsythia, T. denticola, P. intermedia, C. rectus, and F. nucleatum) were observed in either sample type.
3. No serious adverse events were reported during the 12-week intervention period, supporting the safety of the combined probiotic supplementation.
Supplementary materials
The following supplementary materials are available on the journal’s website:
* Supplementary Table S1. Demographics and clinical characteristics at baseline (PP set)
* Supplementary Table S2. Changes in clinical periodontal parameters over 12 weeks (PP set)
* Supplementary Table S3. Serum inflammatory biomarkers over 12 weeks (FA set)
Conceptualization: MY Cho, YY Kim; Data curation: MY Cho; Formal analysis: MY Cho; Funding acquisition: MY Cho, SJ Yang, YY Kim; Investigation: MY Cho, YY Kim; Methodology: MY Cho; Project administration: MY Cho, YY Kim; Resources: MY Cho, JH Eom, SJ Yang, HS Kim; Software: MY Cho; Supervision: MY Cho; Validation: MY Cho; Visualization: MY Cho; Writing-original draft: MY Cho; Writing-review&editing: MY Cho, JH Eom, JW Kim, YW Kim, SJ Yang, JH Lee, HS Kim, J Lee, IH Hwang, YY Kim
S.J. Yang and J.H. Lee are employees of Docsmedi Co., Ltd.\J. Lee is an employee of Daesang Wellife Co., Ltd.\These companies provided funding and supplied the test products. The remaining authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
This study was supported by Daesang Wellife and Docsmedi.
This study was approved by the Institutional Review Board of Apple Tree Medical Foundation (IRB No.\ATDH-2023-0002). Written informed consent was obtained from all participants prior to enrollment. This trial was registered in the Clinical Research Information Service (KCT0009762).
The datasets generated during the current study are available from the corresponding author upon request.
None
1. Kinane DF, Stathopoulou PG, Papapanou PN. Periodontal diseases. Nat Rev Dis Primers 2017;3:17038. https://doi.org/10.1038/nrdp.2017.38
[DOI][PubMed]
2. Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet 2005;366(9499):1809-20. https://doi.org/10.1016/s0140-6736(05)67728-8
[DOI][PubMed]
3. Sherman PR, Hutchens LH Jr, Jewson LG. The effectiveness of subgingival scaling and root planing II. Clinical responses related to residual calculus. J Periodontol 1990;61(1):9-15. https://doi.org/10.1902/jop.1990.61.1.9
[DOI][PubMed]
4. Cobb CM. Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. J Clin Periodontol 2002;29(Suppl 2):6-16. https://doi.org/10.1034/j.1600-051X.29.s2.4.x
[DOI]
5. Teughels W, Feres M, Oud V, Martín C, Matesanz P, Herrera D. Adjunctive effect of systemic antimicrobials in periodontitis therapy: a systematic review and meta-analysis. J Clin Periodontol 2020;47(Suppl 22):257-81. https://doi.org/10.1111/jcpe.13264
[DOI][PubMed]
6. Martin-Cabezas R, Davideau JL, Tenenbaum H, Huck O. Clinical efficacy of probiotics as an adjunctive therapy to non-surgical periodontal treatment of chronic periodontitis: a systematic review and meta-analysis. J Clin Periodontol 2016;43(6):520-30. https://doi.org/10.1111/jcpe.12545
[DOI][PubMed]
7. Borges I, Faveri M, Figueiredo LC, Duarte PM, Retamal-Valdes B, Montenegro SCL, et al. Different antibiotic protocols in the treatment of severe chronic periodontitis: a 1-year randomized trial. J Clin Periodontol 2017;44(8):822-32. https://doi.org/10.1111/jcpe.12721
[DOI][PubMed]
8. GBD 2021 Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance 1990-2021: a systematic analysis with forecasts to 2050. Lancet 2024;404(10459):1199-226. https://doi.org/10.1016/s0140-6736(24)01867-1
[DOI][PubMed][PMC]
9. Matsubara VH, Bandara HM, Ishikawa KH, Mayer MP, Samaranayake LP. The role of probiotic bacteria in managing periodontal disease: a systematic review. Expert Rev Anti Infect Ther 2016;14(7):643-55. https://doi.org/10.1080/14787210.2016.1194198
[DOI][PubMed]
10. Shah MP, Gujjari SK, Chandrasekhar VS. Evaluation of the effect of probiotic (inersan®) alone, combination of probiotic with doxycycline and doxycycline alone on aggressive periodontitis – a clinical and microbiological study. J Clin Diagn Res 2013;7(3):595-600. https://doi.org/10.7860/jcdr/2013/5225.2834
[DOI][PubMed][PMC]
11. Hardan L, Bourgi R, Cuevas-Suárez CE, Flores-Rodríguez M, Omaña-Covarrubias A, Nicastro M, et al. The use of probiotics as adjuvant therapy of periodontal treatment: a systematic review and meta-analysis of clinical trials. Pharmaceutics 2022;14(5):1017. https://doi.org/10.3390/pharmaceutics14051017
[DOI][PubMed][PMC]
12. Nami Y, Haghshenas B, Abdullah N, Barzegari A, Radiah D, Rosli R, et al. Probiotics or antibiotics: future challenges in medicine. J Med Microbiol 2015;64(2):137-46. https://doi.org/10.1099/jmm.0.078923-0
[DOI][PubMed]
13. Meurman JH, Stamatova I. Probiotics: contributions to oral health. Oral Dis 2007;13(5):443-51. https://doi.org/10.1111/j.1601-0825.2007.01386.x
[DOI][PubMed]
14. Lee J, Jang JY, Kwon MS, Lim SK, Kim N, Lee J, et al. Mixture of two Lactobacillus plantarum strains modulates the gut microbiota structure and regulatory T cell response in diet-induced obese mice. Mol Nutr Food Res 2018;62(24):1800329. https://doi.org/10.1002/mnfr.201800329
[DOI][PubMed]
15. Cho MY, Eom JH, Choi EM, Kim JW, Kim YY, Yang SJ, et al. Short-term effects of oral dissolving film on halitosis and oral pathogenic bacteria: a pilot non-randomized controlled trial. Front Microbiol 2025;16:1639960. https://doi.org/10.3389/fmicb.2025.1639960
[DOI][PubMed][PMC]
16. Chan AW, Tetzlaff JM, Altman DG, Laupacis A, Gøtzsche PC, Krleža-Jerić K, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med 2013;158(3):200-7. https://doi.org/10.7326/0003-4819-158-3-201302050-00583
[DOI][PubMed][PMC]
17. Kang MS, Lee DS, Lee SA, Kim MS, Nam SH. Effects of probiotic bacterium Weissella cibaria CMU on periodontal health and microbiota: a randomised, double-blind, placebo-controlled trial. BMC Oral Health 2020;20(1):243. https://doi.org/10.1186/s12903-020-01231-2
[DOI][PubMed][PMC]
18. Jagadeesh MK, Shenoy N, Talwar A, Shetty S. Clinical effect of pro-biotic containing Bacillus coagulans on plaque induced gingivitis: a randomised clinical pilot study. J Health Allied Sci NU 2017;7(3):7-12. https://doi.org/10.1055/s-0040-1708717
[DOI]
19. Germen M, Baser U, Lacin CC, Fıratlı E, İşsever H, Yalcin F. Periodontitis prevalence, severity, and risk factors: a comparison of the AAP/CDC case definition and the EFP/AAP classification. Int J Environ Res Public Health 2021;18(7):3459. https://doi.org/10.3390/ijerph18073459
[DOI][PubMed][PMC]
20. Fleiss JL, Park MH, Chilton NW, Alman JE, Feldman RS, Chauncey HH. Representativeness of the “Ramfjord teeth” for epidemiologic studies of gingivitis and periodontitis. Community Dent Oral Epidemiol 1987;15(4):221-4. https://doi.org/10.1111/j.1600-0528.1987.tb00525.x
[DOI][PubMed]
21. Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol 1967;38(6):610-6. https://doi.org/10.1902/jop.1967.38.6.610
[DOI][PubMed]
22. Jung JS, Choi GH, Lee H, Ko Y, Ji S. The clinical effect of a propolis and mangosteen extract complex in subjects with gingivitis: a randomized, double-blind, and placebo-controlled clinical trial. Nutrients 2024;16(17):3000. https://doi.org/10.3390/nu16173000
[DOI][PubMed][PMC]
23. Han YW. Fusobacterium nucleatum: a commensal-turned pathogen. Curr Opin Microbiol 2015;23:141-7. https://doi.org/10.1016/j.mib.2014.11.013
[DOI][PubMed][PMC]
24. Cicmil S, Cicmil A, Pavlic V, Krunić J, Sladoje Puhalo D, Bokonjić D, et al. Periodontal disease in young adults as a risk factor for subclinical atherosclerosis: a clinical, biochemical and immunological study. J Clin Med 2023;12(6):2197. https://doi.org/10.3390/jcm12062197
[DOI][PubMed][PMC]