
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Hye-Sun Shin1![]() , Ja-Young Moon2
, Ja-Young Moon2![]() , Seon-Ju Sim3
, Seon-Ju Sim3![]()
1Department of Dental Hygiene, Dongnam Health University
2Graduate School, College of Medicine, Yonsei University
3Department of Dental Hygiene, Baekseok University
Correspondence to Seon-Ju Sim, Department of Dental Hygiene, Baekseok University, 1 Baekseok Daehak-ro, Dongnam-gu, Cheonan-si, Chungcheongnam-do, Korea. Tel: +82-10-4902-9394, E-mail: vision1991@bu.ac.kr
Volume 26, Number 3, Pages 339–50, June 2026.
J Korean Soc Dent Hyg 2026;26(3):339–50. https://doi.org/10.13065/jksdh.2026.26.3.7
Received on March 30, 2026, Revised on May 19, 2026, Accepted on June 08, 2026, Published on June 30, 2026.
Copyright © 2026 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0).

Cohort study, Diabetes Mellitus, Epidemiology, IgA nephropathy, Periodontal disease, Recurrent and persistent hematuria
Recurrent and persistent hematuria (RPH) is an important clinical sign of glomerular injury and is frequently observed in the early stages of several renal diseases, including IgA nephropathy (IgAN). Among primary glomerular diseases, IgAN is the most common worldwide and shows marked geographic variation, with a particularly high prevalence in East and Southeast Asian countries, comprising 40–50% of all primary glomerulonephritis cases, compared with 10–20% in North America and Europe and less than 5% in Africa [1].
In Korea, IgAN remains the most common primary glomerulonephritis, accounting for 48.3% of all primary glomerular diseases, according to registry data from the Korean Glomerulonephritis Study Group for 1979–2017 [2]. Although IgAN was initially considered benign, long-term follow-up studies have demonstrated that it follows a slowly progressive course, with up to 50% of patients developing terminal renal failure after several decades [3].
Periodontitis is a multifactorial, biofilm-induced, chronic inflammatory disease of the tooth-supporting tissues, characterized by gingival inflammation, periodontal pocket formation, alveolar bone resorption, and eventual tooth loss. Beyond its local oral effects, periodontitis contributes to low-grade systemic inflammation through three primary mechanisms [4]: dysbiotic subgingival biofilms, chronic release of proinflammatory cytokines [5], and hematogenous dissemination of periodontal pathogens such as Porphyromonas gingivalis and Treponema denticola [6]. These mechanisms have been linked to obesity [7], diabetes mellitus [8], cardiovascular disease [9], and chronic kidney disease [10].
Recent human and animal studies have suggested that periodontal inflammation is linked to glomerular injury and IgAN-related immune mechanisms [11,12]. For example, in some patients with IgAN, increased subgingival colonization by red-complex bacteria has been associated with elevated galactose-deficient IgA1 (Gd-IgA1) levels and more severe proteinuria [11,12], while poor oral hygiene has been linked to lower glomerular filtration rates [13]. Experimental studies have shown that oral infection with specific pathogens may increase Gd-IgA1 production and mesangial inflammation [12,14]. In addition, recent bioinformatic analyses have suggested that shared immune pathways, including dysregulated mucosal T- and B-cell responses, may represent a potential link between periodontitis and glomerular injury [15].
However, a significant gap remains between these mechanistic insights and their validation in population-level epidemiological studies. In large-scale claims-based databases such as the National Health Insurance Service (NHIS) cohort, definitive histopathological records from renal biopsies are not systematically available, making the identification of biopsy-confirmed IgAN challenging. Therefore, validated clinical proxies are needed to address this programmatic constraint.
Clinically, episodic or persistent glomerular hematuria may reflect early glomerular injury and can be observed during the early course of glomerular diseases, including IgAN. Therefore, in nationwide epidemiological studies without biopsy registry data, the ICD-10 code N02, which indicates RPH may serve as a pragmatic claims-based indicator of early glomerular injury. However, because ICD-10 N02-coded RPH is not specific for biopsy-confirmed IgAN and may include hematuria from various glomerular and nonglomerular causes, findings based on this code should be interpreted with caution [16].
Furthermore, systemic metabolic conditions such as diabetes mellitus may act as critical effect modifiers of this association [17]. Hyperglycemia impairs host immune function and promotes proinflammatory cytokine release, which accelerates periodontal tissue destruction and amplifies systemic inflammation [18]. We hypothesized that the altered systemic environment in patients with DM may function as an immunometabolic amplifier, lowering the biological threshold for renal microvascular injury induced by chronic periodontal bacteremia and endotoxemia [19,20]. Thus, a stratified analysis according to diabetes status is essential to determine whether metabolic vulnerability significantly modifies the epidemiological association between PD and early glomerular injury.
The objectives of this retrospective cohort study were twofold: first, to evaluate the 11-year incidence of ICD-10 N02-coded RPH according to baseline periodontal disease status in a large Korean adult population; and second, to assess the potential effect modification by diabetes status and clarify the clinical significance of oral health to renal prognosis.
This retrospective cohort study used data from the National Health Insurance Service–National Sample Cohort (NHIS-NSC), a representative population-based sample drawn from the NHIS in South Korea. The NHIS-NSC comprises an annual, randomized 2.2% sample of the national population—approximately one million individuals per year—covering the period from 2002 to 2015, as detailed previously [21]. Because the NHIS-NSC data were de-identified and administratively collected, the need for individual informed consent was waived. The study protocol was approved by the Baekseok University Institutional Review Board (BUIRB-202001-HR-025).
We initially identified 1,108,369 individuals enrolled in the Korean National Health Insurance Service between 2002 and 2015. To ensure that only incident cases were evaluated, a 3-year baseline and washout period (2002–2004) was applied [22]. The index date was defined as January 1, 2005, and follow-up continued until December 31, 2015. Baseline PD, DM status, and covariates were ascertained during the 2002–2004 baseline period using information available prior to the start of follow-up. During the selection process, we excluded individuals who met the following criteria: (1) age younger than 20 years, (2) a preexisting diagnosis of ICD-10 N02-coded RPH during the washout period, and (3) incomplete claims data for baseline periodontal status or confounding variables. After these exclusions, the final analytical cohort comprised 208,047 participants. This cohort was stratified according to baseline diabetes mellitus status into 180,718 participants without diabetes and 27,329 participants with diabetes. Within each stratum, participants were further classified according to their periodontal disease status: among those without diabetes, 78,660 had no periodontal disease and 102,058 had periodontal disease; among those with diabetes, 9,321 had no periodontal disease and 18,008 had periodontal disease. The final analytical selection process is illustrated in Fig. 1. Eligible participants without baseline ICD-10 N02-coded RPH were followed for up to 11 years to identify newly diagnosed incident cases of ICD-10 N02-coded RPH.
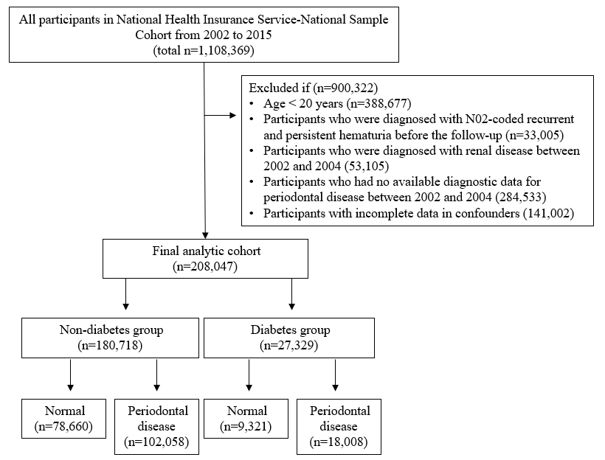
Fig. 1. Flow diagram of the study participants.
Periodontal disease (PD) was assessed by licensed dentists using clinical examination, radiographic evaluation, and diagnostic criteria aligned with the guidelines of the Centers for Disease Control and Prevention and the American Academy of Periodontology [23]. Diagnoses were recorded using ICD-10 codes, including acute gingivitis (K05.0), chronic gingivitis (K05.1), aggressive periodontitis (K05.2), chronic periodontitis (K05.3), unspecified periodontitis (K05.4), other specified periodontal diseases (K05.5), and unspecified periodontal diseases (K05.6). Details of the PD assessment methodology are provided in a previous study [22]. For classification, periodontal status was defined using ICD-10 codes: individuals without any periodontal disease-related codes were classified as the normal group, whereas those with diagnoses ranging from K05.0 to K05.6 were categorized as having periodontal disease [22].
The primary endpoint was new-onset recurrent and persistent hematuria (ICD-10 code N02). Given the absence of biopsy-level granularity in the NHIS-NSC cohort, we employed the N02 classification as a clinical surrogate for early-stage IgAN-related glomerular damage. Consequently, our findings should be interpreted as reflecting N02-coded RPH rather than as definitively biopsy-proven IgAN. An incident event was defined as the first recorded occurrence of ICD-10 code N02 during the follow-up period (2005–2015) among participants without baseline ICD-10 N02-coded RPH.
Sociodemographic variables (age, sex, and household income), health-related lifestyle behaviors (smoking and alcohol use), and systemic health conditions (including hypertension, obesity, and hypercholesterolemia) were documented at baseline (2002–2004) and were included in the statistical analyses as potential confounding factors.
Household income was categorized into quintiles based on the insurance premiums assessed per household. Health-related lifestyle factors were obtained through standardized self-reported questionnaires administered during baseline health screening examinations. Smoking status was classified as current smoker versus nonsmoker (including both never-smokers and former smokers), and alcohol consumption was grouped into five categories: almost never, 2–3 times per month, 1–2 times per week, 3–4 times per week, and almost every day.
Systemic health conditions were identified using health insurance claim data and clinical measurements from the baseline period. Diabetes mellitus was defined by ICD-10 codes E10, E11, E12, E13, and E14 and hypertension by codes I10 and I15. Obesity was defined as a body mass index (BMI) of 25.0 kg/m² or higher [24], calculated using height and weight measurements obtained during baseline health screening. Hypercholesterolemia was defined as a fasting total serum cholesterol level greater than 240 mg/dL [25] at baseline screening.
The baseline characteristics of the study population were summarized according to PD status and stratified according to the presence of DM. Categorical variables are presented as frequencies and percentages, and differences between groups were evaluated using the chi-square test. Statistical significance was defined as a two-sided p-value of < 0.05.
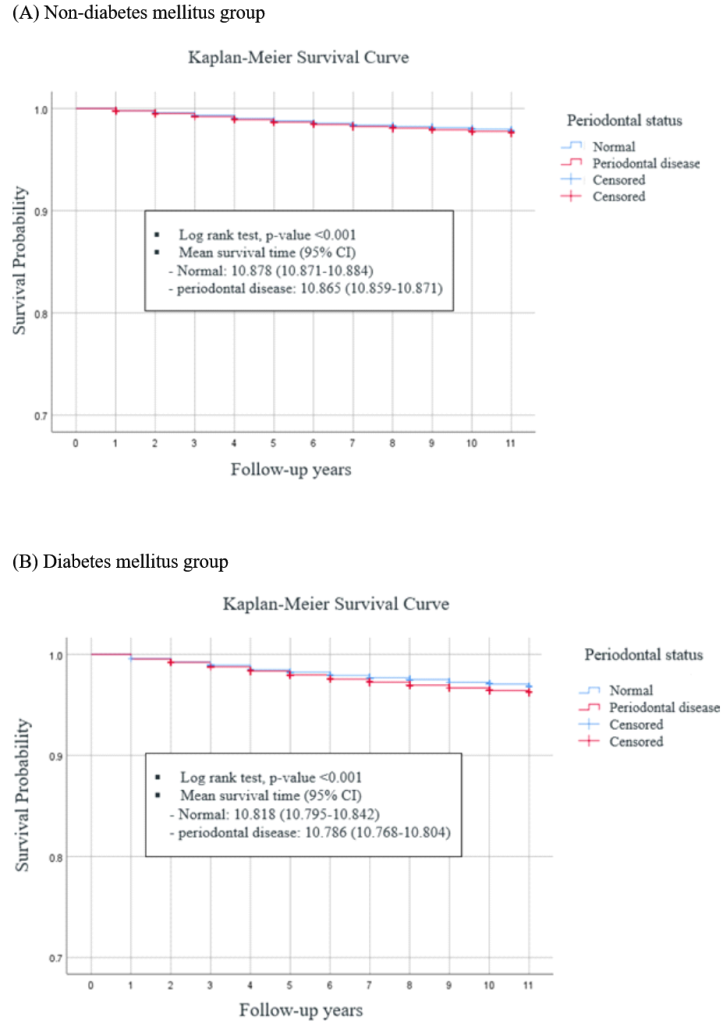
The incidence rate of ICD-10 N02-coded RPH was calculated per 100,000 person-years according to the periodontal disease status. Kaplan–Meier survival curves were generated to estimate the ICD-10 N02-coded RPH-free survival probability over the 11-year follow-up period, stratified by baseline diabetes mellitus status. Differences in survival distributions between the groups with and without periodontal disease were compared using the log-rank test. Time-to-event analyses were based on person-time accrued from the index date (January 1, 2005) until the first occurrence of ICD-10 N02-coded RPH or at the end of follow-up (December 31, 2015), whichever occurred first.
Subgroup analyses were conducted by stratifying participants according to the presence or absence of DM at baseline. Within each stratum, the incidence of ICD-10 N02-coded RPH was compared according to the PD status. To evaluate the epidemiological association between PD and the risk of incident ICD-10 N02-coded RPH, Cox proportional hazards regression analyses were performed. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated across four progressively adjusted models: Model 1 was unadjusted; Model 2 was adjusted for sociodemographic variables (age, sex, and household income); Model 3 was additionally adjusted for lifestyle factors (smoking and alcohol consumption); and Model 4 was adjusted for systemic comorbidities (hypertension, obesity, and hypercholesterolemia). All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
Table 1 presents the baseline characteristics of the 208,047 participants stratified by their baseline DM status and PD status. Among individuals without DM (n = 180,718), 56.5% had PD, whereas PD prevalence was notably higher among individuals with DM (n = 27,329), at 65.9%.
Across both strata, individuals with PD were generally older; for instance, in the DM subgroup, 41.6% of those with periodontal disease were aged ≥60 years, compared with 38.2% of those without PD. Furthermore, a higher prevalence of PD was observed among males and participants with lower household income.
Health-related lifestyle behaviors and systemic comorbidities were also less favorable among patients with PD. Risk behaviors, including smoking and frequent alcohol consumption, and comorbidities such as hypertension, obesity, and hypercholesterolemia, were consistently more prevalent in the PD group, regardless of DM status. For example, within the DM stratum, hypertension affected 43.7% of participants with PD and 41.5% of those without PD. Overall, all observed differences in the baseline characteristics between the groups were statistically significant (p < 0.001, except for hypercholesterolemia, for which p = 0.001).
Table 1. Baseline characteristics of the study participants according to periodontal status (N=208,047)
| Variables | Total N | Non-diabetes group | Diabetes group | p* | ||
|---|---|---|---|---|---|---|
| Normal (n=78,660) | Periodontal disease (n=102,058) | Normal (n=9,321) | Periodontal disease (n=18,008) | |||
| Age group | ||||||
| 20 to 39 | 77,206 | 38,131(48.5) | 36,739(36.0) | 1,047(11.2) | 1,289(7.2) | <0.001 |
| 40 to 59 | 95,080 | 31,685(40.3) | 49,453(48.5) | 4,712(50.6) | 9,230(51.3) | |
| ≥60 | 35,761 | 8,844(11.2) | 15,866(15.5) | 3,562(38.2) | 7,489(41.6) | |
| Sex | ||||||
| Male | 105,768 | 38,305(48.7) | 53,422(52.3) | 4,339(46.6) | 9,702(53.9) | <0.001 |
| Female | 102,279 | 40,355(51.3) | 48,636(47.7) | 4,982(53.4) | 8,306(46.1) | |
| Income** | ||||||
| First quintile | 28,124 | 11,207(14.2) | 13,331(13.1) | 1,260(13.5) | 2,326(12.9) | <0.001 |
| Second quintile | 31,992 | 12,826(16.3) | 15,552(15.2) | 1,287(13.8) | 2,327(12.9) | |
| Third quintile | 44,656 | 17,410(22.1) | 21,851(21.4) | 1,934(20.7) | 3,461(19.2) | |
| Fourth quintile | 47,194 | 17,555(22.3) | 23,335(22.9) | 2,144(23.0) | 4,160(23.1) | |
| Fifth quintile | 56,081 | 19,662(25.0) | 27,989(27.4) | 2,696(28.9) | 5,734(31.8) | |
| Smoking status | ||||||
| No | 142,409 | 53,658(68.2) | 68,624(67.2) | 7,066(75.8) | 13,061(72.5) | <0.001 |
| Yes | 65,638 | 25,002(31.8) | 33,434(32.8) | 2,255(24.2) | 4,947(27.5) | |
| Alcohol consumption | ||||||
| Almost non-drink | 110,548 | 40,011(50.9) | 53,235(52.2) | 6,503(64.9) | 11,249(62.5) | <0.001 |
| 2-3times/month | 39,815 | 16,792(21.3) | 19,617(19.2) | 1,183(12.7) | 2,223(12.3) | |
| 1-2 times/week | 38,097 | 15,314(19.5) | 19,126(18.7) | 1,158(12.4) | 2,499(13.9) | |
| 3-4 times/week | 13,121 | 4,610(5.9) | 6,719(6.6) | 570(6.1) | 1,222(6.8) | |
| Almost every day | 6,466 | 1,933(2.5) | 3,361(3.3) | 357(3.8) | 815(4.5) | |
| Hypertension | ||||||
| No | 177,041 | 71,671(91.1) | 89,787(88.0) | 5,453(58.5) | 10,130(56.3) | <0.001 |
| Yes | 31,006 | 6,989(8.9) | 12,271(12.0) | 3,868(41.5) | 7,878(43.7) | |
| Obesity | ||||||
| No | 141,459 | 54,961(69.9) | 70,143(68.7) | 5,572(59.8) | 10,783(59.9) | <0.001 |
| Yes | 66,588 | 23,699(30.1) | 31,915(31.3) | 3,749(40.2) | 7,225(40.1) | |
| Hyper cholesterolemia | ||||||
| No | 193,666 | 73,429(93.3) | 94,873(93.0) | 8,648(92.8) | 16,716(92.8) | 0.001 |
| Yes | 14,381 | 5,231(6.7) | 7,185(7.0) | 673(7.2) | 1,292(7.2) | |
Data are presented as number and percentage.
*Obtained from chi-square test.
**Divided into quintiles based on the insurance fee imposed on each household.
Bold denotes statistical significance at p<0.05.
During the 11-year follow-up period, 5,996 participants developed incident ICD-10 N02-coded RPH, corresponding to an overall cumulative incidence of 2.4%. The incidence and incidence rates varied notably according to periodontal disease and baseline DM status (Table 2). Among participants without DM, the incidence rate was 191.2 per 100,000 person-years (cumulative incidence, 2.1%) in those without PD and 213.7 per 100,000 person-years (cumulative incidence, 2.4%) in those with PD. Conversely, among participants with DM, the absolute risk was substantially higher, with an incidence rate of 278.9 per 100,000 person-years (cumulative incidence, 3.1%) in those without PD and increased to 330.2 per 100,000 person-years (cumulative incidence, 3.6%) in those with PD.
Kaplan–Meier survival analysis demonstrated a significantly reduced N02-coded RPH-free survival probability among participants with PD compared with those without PD (log-rank test, p < 0.001) (Fig. 2A). This longitudinal divergence in survival distribution according to periodontal status was particularly pronounced in the DM subgroup (Fig. 2B). The survival curves consistently exhibited a steeper decline in the PD subgroups across both strata, reflecting a shorter mean time to the development of incident ICD-10 N02-coded RPH.
| Strata | Periodontal status | n | Number of events(%) | Events/100,000 person-years | Hazard ratio (95% confidence interval) | |||
|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||
| Normal | Normal | 78,660 | 1,657(2.1) | 191.2 | Ref | Ref | Ref | Ref |
| Periodontal disease | 102,058 | 2,399(2.4) | 213.7 | 1.12 (1.05-1.19) | 1.05 (0.98-1.12) | 1.05 (0.98-1.12) | 1.04 (0.98-1.11) | |
| Diabetes mellitus | Normal | 9,321 | 286(3.1) | 278.9 | Ref | Ref | Ref | Ref |
| Periodontal disease | 18,008 | 654(3.6) | 330.2 | 1.19 (1.03-1.37) | 1.17 (1.02-1.35) | 1.17 (1.02-1.35) | 1.17 (1.02-1.35) | |
Independent variable is periodontal status
Model 1: unadjusted association
Model 2: adjusted for age, sex, and income
Model 3: adjusted for age, sex, income, smoking status, and alcohol consumption.
Model 4: adjusted for age, sex, income, smoking status, alcohol consumption, hypertension, obesity, and hypercholesterolemia.
Bold denotes statistical significance at p<0.05.
In the unadjusted analysis (Model 1), baseline PD was significantly associated with incident ICD-10 N02-coded RPH in both the non-diabetic and diabetic strata. Among non-diabetic participants, periodontal disease was associated with a 12% higher hazard of incident N02-coded RPH (hazard ratio [HR] 1.12; 95% confidence interval [CI] 1.05–1.19). Similarly, participants with DM and PD exhibited a 19% higher hazard than participants with DM but without PD (HR, 1.19; 95% CI, 1.03–1.37).
Upon sequential adjustment for covariates, this epidemiological association was attenuated in the non-diabetic group but remained robust among participants with DM. In Model 2 (adjusting for sociodemographic factors) and Model 3 (additionally adjusting for lifestyle behaviors), the association in non-diabetic participants became statistically non-significant (Model 3: HR 1.05; 95% CI 0.98–1.12), whereas it persisted among participants with DM (Model 3: HR, 1.17; 95% CI, 1.02–1.35).
In the fully adjusted analysis (Model 4), which further accounted for systemic comorbidities (hypertension, obesity, and hypercholesterolemia), no statistically significant association was observed among non-diabetic individuals (adjusted HR [aHR], 1.04; 95% CI, 0.98–1.11). In contrast, PD remained independently associated with a modest but statistically significant 17% higher risk of incident ICD-10 N02-coded RPH only within the DM subgroup (aHR, 1.17; 95% CI, 1.02–1.35).
In this large-scale population-based cohort study, we found that periodontal disease (PD) was epidemiologically associated with a higher hazard of incident ICD-10 N02-coded recurrent and persistent hematuria (RPH) over an 11-year follow-up period, particularly in individuals with diabetes mellitus (DM). After full covariate adjustment, this association remained statistically significant only in the DM subgroup, whereas it was attenuated and no longer statistically significant in non-diabetes individuals. To the best of our knowledge, this is the first human cohort study to provide large-scale epidemiological evidence linking PD to the subsequent development of ICD-10 N02-coded RPH, thereby highlighting the potential role of periodontal inflammation in claims-based indicators of early glomerular injury.
Our epidemiological findings align with a growing body of microbiological and immunological research suggesting a structural link between the oral microbiome and IgAN [11,12,15,26–29]. Clinical and 16S rRNA sequencing studies have demonstrated that patients with IgAN have a higher prevalence of severe periodontitis and significant subgingival dysbiosis [27–29]. The translocation of periodontal pathogens such as P. gingivalis, Treponema species, and Campylobacter rectus provides a plausible mechanistic rationale for involvement of the tonsillar-renal axis and activation of aberrant mucosal immunity [11,29]. Notably, P. gingivalis infection induces IgA deposition and mesangial proliferation in animal models [11,14]. At the molecular level, shared immune responses driven by T and B cells [15], along with elevated plasma levels of Gd-IgA1 stimulated by P. gingivalis [12], link oral infections to the core pathogenic features of IgAN. Together, these studies provide biological evidence that persistent periodontal infection may contribute to aberrant mucosal immune responses implicated in early glomerular injury.
This is the first large-scale epidemiological investigation of a human population to test this framework. Our findings suggest that the concurrent presence of DM and PD is associated with an elevated hazard and earlier onset of ICD-10 N02-coded RPH. DM should be considered when evaluating periodontitis-related renal risks because it can exacerbate periodontal pathology and independently contribute to renal injury [19,20]. In DM, impaired neutrophil function and elevated proinflammatory cytokines create a hyperinflammatory subgingival milieu [17,18]. Conversely, chronic periodontal inflammation worsens glycemic indices, potentially amplifying systemic microvascular damage [19,20]. Furthermore, periodontitis has been identified as an independent predictor of macroalbuminuria and the progression to end-stage renal disease in patients with type 2 DM [19]. In the sequentially adjusted models, the effect estimate for PD within the DM stratum remained stable after including demographic, behavioral, and cardiometabolic covariates. This reflects a robust underlying association that is minimally confounded by these factors, justifying the incorporation of diabetes status into early glomerular injury risk assessments.
This study has several notable strengths. It is one of the first large-scale, nationally representative cohort studies with long-term follow-up to evaluate the association between PD and ICD-10 N02-coded RPH as a claims-based indicator of early glomerular injury. We rigorously adjusted for multiple confounders and provided valuable clinical insights through stratification by DM status, successfully bridging the gap between the existing microbiological evidence and human epidemiology.
However, this study has certain limitations. First, defining PD as a single binary variable based on broad ICD-10 codes (K05.0–K05.6) failed to separate mild gingivitis from severe periodontitis. This may have increased clinical heterogeneity, especially among older adults, and may have diluted the association, potentially underestimating the risk of severe periodontitis. Because the NHIS-NSC cohort was established in 2002, PD diagnoses before 2002 were unavailable. Therefore, some participants classified as not having periodontal disease during the baseline period may have had pre-existing PD before cohort entry, which may have introduced exposure misclassification.
Future investigations should aim to refine the exposure definition by utilizing specific dental procedure codes (e.g., simple scaling vs. root planing or periodontal flap surgery) to better capture the clinical severity of periodontitis and evaluate dose-response relationships. Second, the outcomes relied on registry codes without biopsy confirmation, which increased the risk of diagnostic misclassification. Because we defined the endpoint using the ICD-10 N02 code, the outcome should be explicitly interpreted as ICD-10 N02-coded RPH rather than biopsy-confirmed IgAN. This clinical proxy does not strictly confirm biopsy-proven IgAN and may capture a range of glomerular and non-glomerular conditions. Thus, it should be interpreted with caution. Third, potential detection bias cannot be ruled out; patients with periodontal disease may undergo more frequent healthcare interactions, thereby increasing the likelihood of incidental ICD-10 N02-coded RPH detection. Our dataset lacked detailed outpatient visit frequencies to account for this healthcare utilization pattern. Fourth, variables such as hypertension or obesity may act as mediators, which raises the possibility of overadjustment, whereas unmeasured confounders may still exist. This underscores the need for directed acyclic graph-based approaches in future research to optimize covariate selection. Finally, as an observational study, we can report an epidemiological association but cannot establish direct causality or determine the underlying molecular mechanisms linking periodontal inflammation to glomerular injury.
The aim of this nationwide retrospective cohort study was to evaluate the epidemiological association between PD and incident ICD-10 N02-coded RPH, a clinical proxy for early-stage IgAN, over an 11-year follow-up period using NHIS–NSC data. A total of 208,047 adults were evaluated, and Cox proportional hazards models were applied with sequential adjustments for demographic, behavioral, and cardiometabolic covariates.
1. PD is significantly associated with incident N02-coded RPH, particularly in individuals with concurrent DM. After full covariate adjustment, this association remained statistically significant only in the DM subgroup, whereas it was attenuated and no longer statistically significant in non-diabetes individuals.
2. These findings suggest that chronic periodontal inflammation may be epidemiologically linked to incident ICD-10 N02-coded RPH, particularly in the presence of metabolic vulnerabilities, such as DM. However, further studies using more specific renal outcomes are needed before clinical implications can be established.
Conceptualization: SJ Sim, JY Moon; Data collection: SJ Sim, HY Shin; Formal analysis: SJ Sim, HY Shin, JY Moon; Writing-original draft: SJ Sim, JY Moon, HY Shin; Writing-review and editing: SJ Sim, JY Moon, and HY Shin.
The authors declare no conflicts of interest.
This study was conducted with research grant support from Dongnam Health University.
This study was approved by the Institutional Review Board (IRB) of Baekseok University (IRB No.\BUIRB-202001-HR-025).
Data are available from the corresponding author upon reasonable request.
None.
1. Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med 2013;368:2402-14. https://doi.org/10.1056/NEJMra1206793
[DOI][PubMed]
2. Korean Glomerulo Nephritis Study Group. Renal diseases in numbers in Korea 2019. Seoul: The Korean Society of Nephrology Registry Committee; 2019.
3. Pettersson E. IgA nephropathy: 30 years on. J Intern Med 1997;242:349-53. https://doi.org/10.1046/j.1365-2796.1997.00194.x
[DOI][PubMed]
4. Marchesan JT, Girnary MS, Moss K, Monaghan ET, Egnatz GJ, Jiao Y, et al. Role of inflammasomes in the pathogenesis of periodontal disease and therapeutics. Periodontol 2000 2020;82:93-114. https://doi.org/10.1111/prd.12269
[DOI][PubMed]
5. Neurath N, Kesting M. Cytokines in gingivitis and periodontitis: from pathogenesis to therapeutic targets. Front Immunol 2024;15:1435054. https://doi.org/10.3389/fimmu.2024.1435054
[DOI][PubMed][PMC]
6. Graves DT, Corrêa JD, Silva TA. The oral microbiota is modified by systemic diseases. J Dent Res 2019;98:148-56. https://doi.org/10.1177/0022034518805739
[DOI][PubMed][PMC]
7. Nascimento GG, Leite FR, Do LG, Peres KG, Correa MB, Demarco FF, et al. Is weight gain associated with the incidence of periodontitis? A systematic review and meta-analysis. J Clin Periodontol 2015;42:495-505. https://doi.org/10.1111/jcpe.12417
[DOI][PubMed]
8. Sanz M, Ceriello A, Buysschaert M, Chapple I, Demmer RT, Graziani F, et al. Scientific evidence on the links between periodontal diseases and diabetes: consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol 2018;45:138-49. https://doi.org/10.1111/jcpe.12808
[DOI][PubMed][PMC]
9. Schenkein HA, Papapanou PN, Genco R, Sanz M. Mechanisms underlying the association between periodontitis and atherosclerotic disease. Periodontol 2000 2020;83:90-106. https://doi.org/10.1111/prd.12304
[DOI][PubMed]
10. Parsegian K, Randall D, Curtis M, Ioannidou E. Association between periodontitis and chronic kidney disease. Periodontol 2000 2022;89:114-24. https://doi.org/10.1111/prd.12431
[DOI][PubMed]
11. Nagasawa Y, Misaki T, Ito S, Naka S, Wato K, Nomura R, et al. Title IgA nephropathy and oral bacterial species related to dental caries and periodontitis. Int J Mol Sci 2022;23:725. https://doi.org/10.3390/ijms23020725
[DOI][PubMed][PMC]
12. Ito S, Misaki T, Nagasawa Y, Nomura R, Naka S, Fukunaga A, et al. Porphyromonas gingivalis infection in the oral cavity is associated with elevated galactose-deficient IgA1 and increased nephritis severity in IgA nephropathy. Clin Exp Nephrol 2024;28:192-200. https://doi.org/10.1007/s10157-023-02411-4
[DOI][PubMed]
13. Suzuki H, Kiryluk K, Novak J, Moldoveanu Z, Herr AB, Renfrow MB, et al. The pathophysiology of IgA nephropathy. J Am Soc Nephrol 2011;22:1795-803. https://doi.org/10.1681/asn.2011050464
[DOI][PubMed][PMC]
14. Misaki T, Naka S, Wato K, Hatakeyama R, Nagasawa Y, Ito S, et al. Campylobacter rectus in the oral cavity correlates with proteinuria in immunoglobulin A nephropathy patients. Nephron 2018;139:143-9. https://doi.org/10.1159/000487103
[DOI][PubMed]
15. Gao X, Guo Z, Wang P, Liu Z, Wang Z. Transcriptomic analysis reveals the potential crosstalk genes and immune relationship between IgA nephropathy and periodontitis. Front Immunol 2023;14:1062590. https://doi.org/10.3389/fimmu.2023.1062590
[DOI][PubMed][PMC]
16. Sumantri AP, Kim CK, Chen Q, Cannizzaro NT, Sim JJ. Accuracy of ICD-10 coding for identifying immunoglobulin A nephropathy (IgAN) prior to 2023. Clin Kidney J 2025;18:sfaf327. https://doi.org/10.1093/ckj/sfaf327
[DOI][PubMed][PMC]
17. Mealey BL, Ocampo GL. Diabetes mellitus and periodontal disease. Periodontol 2000 2007;44:127-53. https://doi.org/10.1111/j.1600-0757.2006.00193.x
[DOI][PubMed][PMC]
18. Taylor GW. Bidirectional interrelationships between diabetes and periodontal diseases: an epidemiologic perspective. Ann Periodontol 2001;6:99-112. https://doi.org/10.1902/annals.2001.6.1.99
[DOI][PubMed]
19. Effect of periodontitis on overt nephropathy and end-stage renal disease in type 2 diabetes. Diabetes Care 2007;30:306-11. https://doi.org/10.2337/dc06-1184
[DOI][PubMed]
20. Fisher MA, Taylor GW, Shelton BJ, Jamerson KA, Rahman M, Ojo AO, et al. Periodontal disease and other nontraditional risk factors for CKD. Am J Kidney Dis 2008;51:45-52. https://doi.org/10.1053/j.ajkd.2007.09.018
[DOI][PubMed]
21. Lee J, Lee JS, Park SH, Shin SA, Kim K. Cohort profile: the National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int J Epidemiol 2017;46:e15. https://doi.org/10.1093/ije/dyv319
[DOI][PubMed]
22. Shin HS, Hong MH, Moon JY, Sim SJ. Periodontal disease could be a potential risk factor for non-alcoholic fatty liver disease: an 11-year retrospective follow-up study. Clin Oral Investig 2022;26:5503-14. https://doi.org/10.1007/s00784-022-04518-6
[DOI][PubMed]
23. Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol 1999;4:1-6. https://doi.org/10.1902/annals.1999.4.1.1
[DOI][PubMed]
24. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004;363:157-63. https://doi.org/10.1016/s0140-6736(03)15268-3
[DOI][PubMed]
25. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285:2486-97. https://doi.org/10.1001/jama.285.19.2486
[DOI][PubMed]
26. Stamellou E, Seikrit C, Tang SCW, Boor P, Tesař V, Floege J, et al. IgA nephropathy. Nat Rev Dis Primers 2023;9:67. https://doi.org/10.1038/s41572-023-00476-9
[DOI][PubMed]
27. Cao YL, Qiao M, Xu ZH, Zou GM, Ma LL, Li WG, et al. [The clinical study of IgA nephropathy with severe chronic periodontitis and aggressive periodontitis]. Zhonghua Yi Xue Za Zhi 2016;96:9-13.
[DOI]
28. Cao Y, Qiao M, Tian Z, Yu Y, Xu B, Lao W, et al. Comparative analyses of subgingival microbiome in chronic periodontitis patients with and without IgA nephropathy by high throughput 16S rRNA sequencing. Cell Physiol Biochem 2018;47:774-83. https://doi.org/10.1159/000490029
[DOI][PubMed]
29. Jing L, Adelibieke Y, Feifan G, Chen D, Yuanming Z. Distribution of subgingival bacteria in chronic periodontitis patients correlated with IgA nephropathy. Clin Lab 2024;70: 10.7754/Clin.Lab.2023.230316. https://doi.org/10.7754/Clin.Lab.2023.230316
[DOI]