
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Weeks in Review
Weeks to Publication
Journal of Korean Society of Dental Hygiene![]() Open access, Peer Reviewed
Open access, Peer Reviewed
pISSN 2287-1705, eISSN 2288-2294
Yun-Woo Kim![]() , Do-Seon Lim
, Do-Seon Lim![]() , Hee-Jung Lim
, Hee-Jung Lim![]() , Im-Hee Jung
, Im-Hee Jung![]()
Department of Dental Hygiene, Graduate School, Eulji University
Correspondence to Im-Hee Jung, Department of Dental Hygiene, Graduate School, Eulji University, 553 Sanseong-daero, Sujeong-gu, Seongnam-si, Gyeonggi-do, 13135, Korea. Tel: +82-31-740-7247, Fax: +82-31-740-7352, E-mail: Jungih@eulji.ac.kr
Volume 24, Number 4, Pages 271-80, August 2024.
J Korean Soc Dent Hyg 2024;24(4):271-80. https://doi.org/10.13065/jksdh.20240401
Received on May 14, 2024 , Revised on June 14, 2024, Accepted on June 21, 2024, Published on August 30, 2024.
Copyright © 2024 Journal of Korean Society of Dental Hygiene.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License(http://creativecommons.org/licenses/by-nc/4.0)

Objectives: This study aimed to test whether the digital competence of dental hygienists can affect their intraoral scanning potential in terms of scan time and error. Methods: Dental hygienists and dental hygiene students who had never used an intraoral scanner were surveyed to determine their digital competence. Individual data collected using an intraoral scanner was compared with reference data collected using a model scanner to identify scanning errors, and participants’ scanning times were measured. Results: A significant decrease in scanning time was observed as the overall level of digital competence increased. The increase in digital skills and digital knowledge led to a decrease in scanning time by 3.73 and 3.98 minutes, respectively. Conclusions: This study found that digital competence was associated with reduced scan times, but less so with scan errors. This may be due to recent advances in scanning software, and future studies may need to develop a digital competence assessment tool that is more appropriate for the dental field.
Data accuracy, Dental impression technique, Digital health, Professional competence, Time and motion studies
In the era of the fourth industrial revolution driven by advanced information and communication technology, efforts are being made worldwide, including in Korea, to integrate digital technologies across various sectors of society [1,2]. The introduction of oral scanners represents one of the significant changes in digitized dental care [3]. Oral scanning is a modern method used for recording the positive and negative forms of oral tissues to fabricate dental prostheses [4]. Instead of using traditional impression materials, this technique captures intraoral surface data using light sources and forms a three-dimensional image [5]. Known as digital impression taking, oral scanning offers advantages over traditional methods by reducing patient discomfort and potentially lowering costs in the long run [4]. Furthermore, it facilitates easy data storage, improves the clinical environment, and has positive effects on dental care, leading to increased use of oral scanners [5,6].
Lack of competence in the acquisition of these digital impressions can lead to long scan times, and prolonged scans can be uncomfortable for patients [5]. Longer scan times result in a higher number of captures, which lead to more errors and reduce the accuracy of the data [7]. Therefore, to ensure the precise fabrication of dental prostheses, it is crucial to have the capability to perform oral scanning accurately within a short duration.
Digital competence refers to a set of attitudes, skills, and knowledge required to use various digital media and information and communication technologies [8]. This concept extends beyond the ability to operate digital devices to include managing digital information and utilizing technologies more broadly. According to Jung [9], enhancing users’ digital competence is essential for the effective use of digital devices. Therefore, it is necessary to investigate whether digital competence affects scanning ability in the context of oral scanners. However, to the best of our knowledge, no studies have been conducted in the field of dentistry on the impact of digital competence on the level of oral scanning, except for a study that investigated the association between computeraided design (CAD) programs and digital literacy [10].
Therefore, this study aims to determine the effect of digital competence on scan time and error among dental hygienists and dental hygiene students.
This study was conducted on dental hygienists or dental hygiene students who had never used an oral scanner before. Sample size was calculated using a dedicated program (G*power 3.1.9.7, Germany) with an effect size of 0.35, a significance level of 0.05, and a power of 85%. Thirty-five participants recruited via announcements were included in this study.
This study was conducted from July 2023 to September 2023 with ethical approval (EU23-013) from the Institutional review board (IRB) of Eulji University. The process of this study is shown in <Fig. 1>.
First, digital competence was measured using a self-report survey. The scale was adapted from a previous study [11] with some modifications for this study (Cronbach’s α=0.903-0.978). It consisted of 29 questions in total, including ‘digital attitudes’, ‘digital skills (basic skills, life utilization, production sharing)’, and ‘digital knowledge (information judgment, security and safety)’; the reliability (Cronbach’s α) in this study was 0.754 for digital attitudes, 0.844 for digital skills, and 0.758 for digital knowledge. Each question was rated on a 4-point Likert scale, with higher scores indicating higher digital competence.
We provided theoretical and demonstration training on the definition, structure, working principle, operating methods, and strategies of oral scanners to participants who had never used an oral scanner before. Subsequently, the participants practiced using a real oral scanner (i700, Medit, Seoul, Korea) and an oral model (TKY-403, TuoKang Medical, China).
The participants were scanned a total of three times using the same oral scanner and oral model used in the previous training. Each scan was taken of the maxilla first, followed by the mandible, and the sequence was as per the manufacturer’s instructions: occlusal surface of the right posterior teeth–incisal edge of the anterior teeth–occlusal surface of the left posterior teeth–lingual surface of the left posterior teeth–lingual surface of the anterior teeth–lingual surface of the right posterior teeth–buccal surface of the right posterior teeth–labial surface of the anterior teeth–buccal surface of the left posterior teeth–occlusal surfaces of both sides. Scanning time was measured from the time the participant first pressed the ‘Start scan’ button to the time the last data were saved, for each of the first and third occlusal planes. The training, scanning, and measurement processes were all performed in a uniform manner by the same researcher.
The reference images for error analysis were acquired with a model scanner (Freedom UHD, DOF Inc, CA, USA). The oral model used was the same as the model used to measure the scan time, and the storage format of the reference image and 1-3 individual images was unified in standard tessellation language (STL) format. All processes related to file extraction and analysis were performed by the same researcher using a uniform method.
The error relative to the reference image was then analyzed in three dimensions for each of the individual scanned images (primary and secondary scan errors) and for the image merged from the individual scans into one (average scan error). The threedimensional error analysis was performed using Geomagic Control X (3D systems, USA). In the program, the error was displayed as a color map and root mean square (RMS), and the color spacing on the color map was set to 100 μm.
The normality of each dataset was confirmed using the Shapiro-Wilk test. Descriptive statistics were used to summarize the general characteristics of the participants, digital competence, scan time, and scan errors. Differences in these dependent variables based on the general characteristics of the participants were analyzed using independent t-tests and one-way analysis of variance (ANOVA). Differences in scan time and errors according to the number of scans were analyzed using repeated measures ANOVA. Differences in scanning ability based on levels of digital competence were analyzed using independent t-tests. The impact of general characteristics and digital competence on scan time and scan errors was analyzed using multiple regression analysis. The data were statistically analyzed using IBM SPSS program (ver. 25.0; IBM Corp., Armonk, NY, USA), with the significance level set at 0.05.
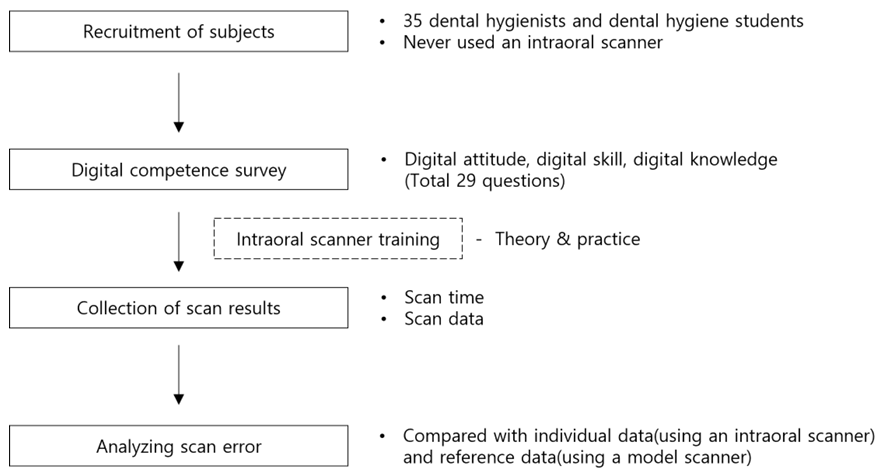
Fig. 1. Experiment procedure
The majority of participants were female (89%), with 83% under 30 and 17% over 30. In terms of education, 51% were in college, 32% graduated from a 3-year or 4-year college, and 17% had a master’s degree or higher. In terms of years of experience, 51% were college students, 29% had 1-3 years of experience, and 20% had ≥ 4 years of experience. Finally, 71% had a computer certification <Table 1>.
Differences in digital competence, scan time, and scan error according to general characteristics were analyzed, and age was the only significant factor. Specifically, digital competence and scan time significantly differed according to age (p<0.05), but scan error did not (p>0.05). Digital competence was higher in the younger age group, with a score of 3.09 for those under 30 and 2.74 for those aged 30 years and over (p<0.05). The mean scan time was shorter in the younger age group, with a score of 22.12 minutes for those under 30 and 26.45 minutes for those aged 30 years and over (p<0.01) <Table 1>.
The mean overall digital competence score was 3.03. More specifically, the scores were 2.76 for digital attitude, 3.48 for digital skills, and 3.16 for digital knowledge. In the digital skills domain, the score was the highest for basic skills (3.59) and the lowest for production sharing (3.04). In the digital knowledge domain, the score was 3.22 for information judgment and 3.10 for security and safety.
Table 1. Digital competence, scan time, and scan error by general characteristics
| Characteristics | Division | N(%) | Average digital competence (score) | Average scan time (min) | Average scan error in maxillary (μm) | Average scan error in mandible (μm) | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean±SD | p* | Mean±SD | p* | Mean±SD | p* | Mean±SD | p* | |||
| Sex | Male | 4(11.0) | 3.22±0.21 | 0.316 | 19.57±1.79 | 0.055 | 28.00±0.84 | 0.448 | 28.20±0.63 | 0.757 |
| Female | 31(89.0) | 3.01±0.40 | 23.29±3.65 | 28.26±0.62 | 28.07±0.81 | |||||
| Age (yr) | <30 | 29(83.0) | 3.09±0.37 | 0.038 | 22.12±3.48 | 0.007 | 28.20±0.65 | 0.529 | 28.02±0.83 | 0.137 |
| ≥30 | 6(17.0) | 2.74±0.33 | 26.45±2.31 | 28.38±0.63 | 28.40±0.46 | |||||
| Educational level | Students | 18(51.0) | 3.02±0.41 | 0.650 | 22.68±3.59 | 0.870 | 28.06±0.64 | 0.237 | 27.99±0.89 | 0.773 |
| Graduate | 11(32.0) | 3.10±0.42 | 23.36±4.28 | 28.38±0.62 | 28.20±0.80 | |||||
| ≥Graduate school | 6(17.0) | 2.92±0.25 | 22.52±3.24 | 28.48±0.61 | 28.15±0.39 | |||||
| Clinical experience (yr) | None | 18(51.0) | 3.02±0.41 | 0.538 | 22.68±3.59 | 0.071 | 28.06±0.64 | 0.157 | 27.99±0.89 | 0.775 |
| 1-3 | 10(29.0) | 3.13±0.16 | 21.38±3.37 | 28.54±0.53 | 28.20±0.64 | |||||
| ≥4 | 7(20.0) | 2.91±0.55 | 25.47±3.34 | 28.24±0.68 | 28.16±0.77 | |||||
| Computer-related certifications | Yes | 25(71.0) | 3.08±0.39 | 0.282 | 22.60±3.62 | 0.515 | 28.14±0.63 | 0.183 | 28.03±0.80 | 0.554 |
| No | 10(29.0) | 2.92±0.36 | 23.52±3.93 | 28.46±0.63 | 28.21±0.78 | |||||
| Total / Average | 35(100.0) | 3.03±0.39 | 22.86±3.67 | 28.23±0.64 | 28.08±0.79 | |||||
*by t-test or ANOVA
Scan time was 25.20 minutes for the first scan, 22.60 minutes for the second scan, and 20.80 minutes for the third scan, showing a significant decrease in scan time with increasing number of scans performed (p<0.001). Maxillary scan error was 28.39 μm for the first scan, 28.15 μm for the second scan, and 27.67 μm for the third scan (p<0.001), and the mandibular scan error was 28.09 μm for the first scan, 28.05 μm for the second scan, and 27.77 μm for the third scan (p<0.05), showing slight decreases in error with increasing number of scans <Table 2>.
Table 2. Scan time and errors depending on the number of scans
Unit: Mean±SD
| Number of scans | Scan time (min) | Scan error (μm) | |
|---|---|---|---|
| Maxillary | Mandible | ||
| 1st | 25.20±4.88a | 28.39±0.65a | 28.09±0.49a |
| 2nd | 22.60±3.73b | 28.15±0.88ab | 28.05±0.65a |
| 3rd | 20.80±3.69c | 27.67±0.99b | 27.77±0.63a |
| p* | <0.001 | <0.001 | 0.039 |
*by one-way repeated measures ANOVA
a,b,cThe same characters was not significant
Differences in scan time and scan error according to digital competence were analyzed. After dividing the participants into two groups based on the mean score of overall digital competence (3.03), we found a statistically significant difference in scan time: 21.02 minutes for the high score group and 24.60 minutes for the low score group (p<0.01). However, no significant difference was observed in the upper and lower scan errors between the groups (p>0.05) <Table 3>.
Table 3. Intraoral scanning skills by digital competence
Unit: Mean±SD
| Variables | Average scan time (min) | Average scan error (μm) | |
|---|---|---|---|
| Maxillary | Mandible | ||
| High | 21.02±3.61 | 28.11±0.71 | 27.95±0.94 |
| Low | 24.60±2.85 | 28.34±0.55 | 28.20±0.62 |
| p* | 0.003 | 0.287 | 0.358 |
*by t-test, Variables were divided based on the mean score of digital competence (3.03 out of 4).
The predictors of average scan time and error were analyzed using regression analysis. First, none of the general characteristics predicted scan time or error, but digital skills and knowledge scores predicted mean scan time. That is, the mean scan time decreased by 3.73 minutes and 3.98 minutes with 1-point increase in digital skills score (p<0.05) and digital knowledge score (p<0.01), respectively. The model explained 60.0% of the variance, and variance inflation factor (VIF) was under 10, confirming the absence of multicollinearity (p<0.001). On the other hand, none of the general characteristics and digital competence factors predicted mean scan error (p>0.05) <Table 4>.
Table 4. Factors influencing average scan time
| Variables | Division | B | SE | β | t | p* |
|---|---|---|---|---|---|---|
| (constant) | 49.951 | 7.572 | 6.597 | <0.001 | ||
| Sex (male=0) | Female | 1.184 | 1.377 | 0.104 | 0.860 | 0.398 |
| Age | 1.284 | 1.995 | 0.142 | 0.643 | 0.526 | |
| Educational level (student=0) | Graduate | 0.765 | 1.136 | 0.098 | 0.674 | 0.507 |
| ≥Graduate school | -1.212 | 1.643 | -0.126 | -0.738 | 0.467 | |
| Clinical experience (none=0) | ≥4 years | -0.039 | 0.185 | -0.053 | -0.210 | 0.835 |
| Computer-related certifications (no=0) | Yes | 0.435 | 1.149 | 0.054 | 0.378 | 0.708 |
| Attitude | -0.732 | 0.794 | -0.116 | -0.922 | 0.365 | |
| Skill | -3.726 | 1.717 | -0.343 | -2.170 | 0.040 | |
| Knowledge | -3.981 | 1.330 | -0.463 | -2.992 | 0.006 | |
| F = 6.663 (p < 0.001), R = 0.840, adjusted R2 = 0.600, DW = 1.967 | ||||||
*by multiple regression analysis
Currently, digital devices are used in many fields, including dentistry [3], and digital competence can influence the efficient use of digital devices [9]. This study aimed to determine whether the digital competence of operators influences their ability to use an intraoral scanner. For this purpose, scan times were measured among dental hygienists and dental hygiene students with no prior experience using intraoral scanners. Additionally, scan errors were assessed by comparing the individual data obtained from the intraoral scanner with the reference data acquired using a model scanner, leading to the following results.
The mean digital competence scores of the participants in this study were 2.7 for attitude, 3.5 for skills, and 3.2 for knowledge. According to Park and Kang [11], the digital competence level of the general population was lower than that of the participants in this study, with an attitude score of 2.6, skill score of 2.6, and knowledge score of 2.4. This difference may be attributed to the fact that the average age of the study participants was 25 years, and they were more familiar with digital equipment and environments due to their specialization in dentistry, unlike the general population in their 40s surveyed in previous studies.
In terms of digital competence, scan time, and errors based on the general characteristics of the participants, digital competence and scan time significantly differed only with respect to age. Specifically, the group under 30 years of age had statistically significantly higher digital competence scores and shorter average scan times than did the group aged 30 years and above. Previous studies on digital competence [12,13] also found that younger groups had higher competence scores and were more adept at handling devices, which was attributed to differences in device adaptability and educational effectiveness across age groups [12]. Therefore, it is essential to consider age when addressing digital competence and the use of intraoral scanners. For older individuals, additional time for device adaptation should be provided in training or research contexts.
In terms of scan times according to digital competence, we found that the average scan time was significantly shorter in the high competence group. Previous studies have reported that an increase in scan time can lead to inaccurate scans due to increased number of scans and accumulated errors [7]. Therefore, the decrease in mean scan time observed in this study can be attributed to a relatively higher ability to utilize the scanner, which is influenced by digital competence. Jung [9] highlights the importance of improving digital competence of the operator in order to facilitate effective digital device use. Park [14] suggests that high digital competence enables faster perception and response to uncertain environments, because it enables faster acquisition and analysis of information. Therefore, the lower scan times in the high digital competence group found in this study may be due to their ability to perceive and respond quickly.
On the other hand, no significant relationship was found between digital competence scores and scanning errors. Previous studies [15] have shown that recent developments in scanning software have incorporated artificial intelligence and automatic segmentation of teeth, which has reduced the variation between scanner users. In this study, we used the latest oral scanner, and it is likely that these new technologies contributed to the lack of differences in scanning error among the participants.
Regarding the factors that contribute to shorter scan times, we found that the skills and knowledge domains of digital competence significantly predict shorter scan times. A study by Son and Lee [10] found that higher digital literacy, which includes both technical and knowledge aspects, can reduce the time spent on devices. Furthermore, Min and Shin [16] found a significant correlation between digital media utilization and digital skills and knowledge. To enhance oral scanning abilities, digital skills and knowledge competence should be improved through targeted support and education. On the other hand, there was no significant correlation between scan time and digital attitude [16]. This might be because actual device usage is less related to digital attitude. Nevertheless, a high digital attitude can increase the recognition of the importance of the digital environment and encourage active participation in device usage. Therefore, digital attitude should still be considered [17], and education aimed at fostering digital attitude is needed.
Taken together, the results show that scanning time is shorter in operators under age 30 and with increasing digital skills and knowledge scores. Therefore, users aged 30 years old and over who want to improve their oral scanning skills should invest more time cultivating digital skills and knowledge as well as device training and adaptation training. However, this study used a measurement tool developed in a previous study [11] to measure digital competence, and the items are related to general digital devices rather than dental-specific devices. Therefore, developing a digital competence measurement tool tailored to the dental field is necessary for directly related results. In addition, we cannot exclude the influence of learning effects due to the fact that the three scans were performed in the same environment. Therefore, we suggest that future studies should experiment with different measurement environments between the first and third scans to control for the confounding factors. Finally, the study’s age range of 21-42 years may have influenced the results; thus, future studies should include a broader age range. Despite these limitations, this study is the first to confirm the influence of digital competence on oral scanner competency, and we hope that the findings serve as valuable data for fostering digital competence and improving oral scanner utilization among dental hygienists.
This study analyzed the effect of digital competence on scan time and error in dental hygienists and dental hygiene students with no prior experience using an intraoral scanner. The conclusions of this study are as follows:
1. Digital competence and scan time significantly differed according to age (p<0.05).
2. Scan time was significantly shorter in the high digital competence group (p<0.01).
3. Digital skills (p<0.05) and digital knowledge (p=0.01) were identified as significant predictors of mean scan time and explained 60.0% of the variance.
These results highlight the need to improve digital competence to reduce scan times for intraoral scanners. When disseminating education about intraoral scanners, it is essential to emphasize digital skills and knowledge. We hope these insights contribute to fostering digital competence and enhancing oral scanner utilization among dental hygienists.
Conceptualization: YW Kim, IH Jung; Data collection: YW Kim, IH Jung; Formal analysis: YW Kim, IH Jung; Writing-original draft: YW Kim, IH Jung; Writing-review & editing: DS Lim, HJ Lim, IH Jung
The authors declared no conflicts of interest.
None.
This study was approved by the Institutional Review Board (IRB) of Eulji University (EU23-013).
None.
None.
1. OECD. Measuring the digital transformation. Paris: OECD; 2019: 1-260.
2. National research council for economics, humanities and social sciences. Designing the future of Korea during the great transformation. Sejong: National Research Council for Economics, Humanities and Social Sciences; 2022: 1-347.
3. Kim YS, Park HS, Ku IY. Perceptions of dental hygienists toward digital dentistry. J Korean Soc Dent Hyg 2013;13(6):909-16. https://doi.org/10.13065/jksdh.2013.13.06.909
[DOI]
4. Kim CH. Impressions for complete dentures. J Kor Dent Assoc 1993;31(1):30-3.
5. Kim RW, Jang GW, Heo YR, Son MK. Understanding and application of digital impression in dentistry. J Korean Acad Prosthodont 2014;41(4):253-61. https://doi.org/10.14815/kjdm.2014.41.4.253
[DOI]
6. Kim JH, Lee HJ, Go SM, Kim HC. A survey on dental personnel’s perceptions of digital dentistry and dental digital equipment. J Kor Dent Assoc 2021;59(5):262-74. https://doi.org/10.22974/jkda.2021.59.5.001
[DOI]
7. Kang SH, Fang JW, Seung MJ, Hwang CH, Kim DH, Choi BH. Immediate restorations in a fully edentulous patient utilizing digital system: a case report. J Korean Acad Prosthodont 2015;53(2):157-66. https://doi.org/10.4047/jkap.2015.53.2.157
[DOI]
8. Choi SY. A study on the digital competence for the fourth industrial revolution. The Journal of Korean Association of Computer Education 2018:21(5):25-35. https://doi.org/10.32431/kace.2018.21.5.003
[DOI]
9. Jung JH. Information and communication technology (ICT) challenges for safe and effective utilization of digital therapeutic devices. Seoul: National Assembly Research Service; 2023: 1-4.
10. Son KBD, Lee KB. Effect of computer literacy on the working time of the dental CAD software program. J Prosthodont Res 2021;65(2):255-60. https://doi.org/10.2186/jpr.JPR_D_20_00030
[DOI][PubMed]
11. Park SM, Kang MW. Basic research on digital competence survey of Seoul residents. Seoul: Seoul Digital Foundation; 2021: 1-79.
12. Song JH, Kim DW. A study on ability and utilization of smart devices for the disabled: focusing on the effect of education for smart device utilization. Informatization Policy 2014;21(2):67-88. https://doi.org/10.22693/NIAIP.2014.21.2.067
[DOI]
13. Oh JA, Yoo JW. A study on the effects of digital literacy on the psychological wellbeing and life satisfaction of the elderly. Korean Public Management Review 2018;32(2):319-44. https://doi.org/10.24210/kapm.2018.32.2.013
[DOI]
14. Park SH. The effect of CEO’s digital competence on the innovation activities of companies. JHRMR 2021;28(4):73-101. https://doi.org/10.14396/jhrmr.2021.28.4.73
[DOI]
15. Vinayahalingam S, Kempers S, Schoep J, Hsu TMH, Moin DA, Cinneken B, et al. Intra-oral scan segmentation using deep learning. BMC Oral Health 2023;23(1):643-51. https://doi.org/10.1186/s12903-023-03362-8
[DOI][PubMed][PMC]
16. Min JH, Shin DJ. The relationship between early childhood teachers’ digital technology knowledge, skill, attitude and digital media utilization. JCME 2023;22(1):77-104. https://doi.org/10.21183/kjcm.2023.03.22.1.77
[DOI]
17. Seo SH, Cho BY, Kim JY, Kim JY, Kim HD, Go JA, et al. Korean elementary students’ digital literacy attitude. Journal of Elementary Korean Education 2016;61(1):153-88. https://doi.org/10.22818/jeke.2016..61.153
[DOI]