Introduction
The decline in oral muscle strength that comes with aging can lead to issues with chewing function, which is essential for digestion. In severe cases, this can result in dysphagia and aspiration pneumonia [1]. Additionally, diminished chewing ability can cause nutritional deficiencies, adversely affecting overall health, quality of life, and satisfaction [2]. Therefore, maintaining oral health in older adults requires not only the prevention of oral diseases but also the enhancement of oral function. It is crucial to boost oral muscle strength through strengthening exercises before significant weakening occurs.
In 2005, Robbins et al. [3] developed a tongue resistance exercise designed to enhance oral muscle strength, demonstrating its effectiveness in older adults. In 2019, Takahashi and Satoh [4] showed improvements in swallowing and feeding functions following gum chewing exercises aimed at strengthening both intra- and extra-oral muscles in healthy adults without oro-maxillary dysfunction. Korean studies from 2017 and 2019 also indicated that tongue-palate resistance exercises were beneficial in fortifying oropharyngeal muscles and enhancing swallowing function in older adults [5,6]. A study in 2020 [7] reported that two different tongue exercise programs led to increased oral muscle strength and salivation. Furthermore, research in 2022 [8] found that combining mouth gymnastics with tongue strength training effectively improved oral muscle function, increased saliva production, alleviated dysphagia, and enhanced articulation in older adults. Despite these exercises’ effectiveness in strengthening oral muscles, their awareness remains limited. This study initially explored the perceptions and practices surrounding oral muscle strength training among dental care professionals [9] and the general public [10]. Findings revealed that both groups acknowledged the importance of oral muscle strength training but cited a scarcity of information and educational resources. They were also open to participating in such training if it was not limited by time and space constraints. Therefore, the oral health community should focus more on the efficacy of oral strength training and develop programs tailored to the specific needs of the target audience.
Virtual reality (VR)-based educational content, which offers users the opportunity to indirectly experience real-life scenarios, has become an innovative alternative to traditional educational methods in medicine, including rehabilitation and brain training [11]. VR technology enables repetitive training without the limitations of time and space [12], and recently, educational materials using VR have been developed in the field of dentistry [13,14]. However, there is a scarcity of VR-based educational content for the general public, especially materials specifically designed for oral muscle strength training.
To develop content for oral muscle strength training using VR technology, this study investigated the awareness and demand for VR-based training among dental professionals [15] and the general public [16] and also sought expert opinions on the development of such content. During this exploration, it became clear that certain movements could not be effectively trained through VR alone. As a result, we incorporated augmented reality (AR), which can be operated on a smartphone, to accommodate these specific movements. Furthermore, the study aimed to assess improvements in oral functions among older adults after they participated in the VR- and AR-based oral muscle strength training programs.
Methods
1. Participants
This study employed a controlled, pretest-posttest design to evaluate the effects of oral muscle-strengthening training. Participants were randomly assigned to either the experimental or control group before the pretest and posttest assessments were conducted.
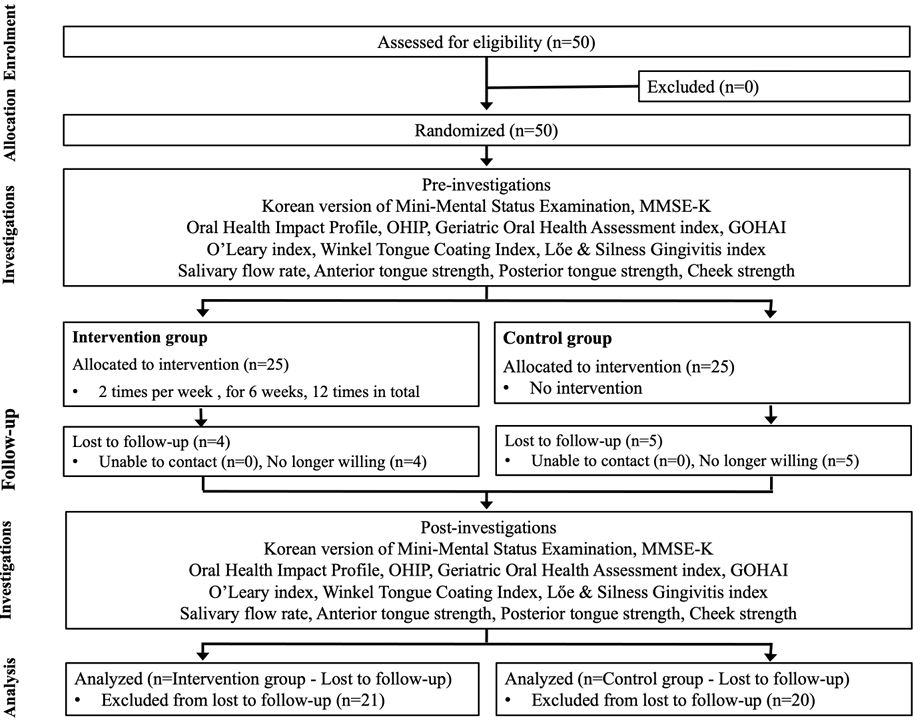
The Institutional Review Board (IRB approval number: SHIRB-202403-HR-224-02) approved the study, ensuring ethical protection for the participants. Individuals aged 65 and older were recruited from senior welfare centers in the metropolitan area through non-probability sampling methods. Eligibility criteria included providing informed consent, being able to communicate, being mobile, and not participating in any other oral health intervention programs. The sample size was determined using G*power 3.1.9.4 for Windows, based on a mean difference test to detect improvements in oral function with a significance level of 0.05, a power of 0.8, and an effect size of 0.8. The calculation resulted in a minimum required sample size [17] of 21 participants per group, totaling 42 participants. However, to account for potential dropouts, 50 subjects were initially selected, with 25 allocated to each group (experimental and control). After removing those who withdrew from the study and those in the experimental group who did not complete all 12 sessions of the intervention, the final analysis included 21 participants in the experimental group and 20 in the control group (Fig. 1).
2. Methods
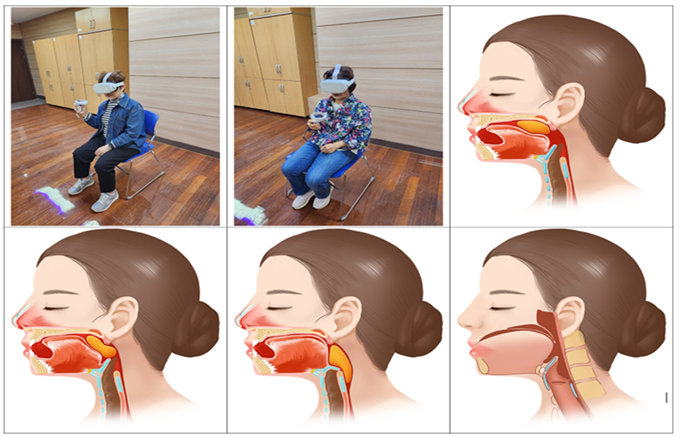
First, we developed VR- and AR-based content for oral strength training. The VR content covered three topics: swallowing, premeal stretching, and gum massage, while the AR content focused on mouth and tongue exercises. This oral muscle strength training was conducted 12 times over 6 weeks, from late August 2023 to early October 2023. The sessions took place at the participants’ organizations, and each lasted approximately 60 minutes.
Before commencing the VR training, trainers familiarized themselves with the content’s usage and sequence to ensure ease of use for the older adult participants. Experts also calibrated the content to align with the user’s gaze before starting, and participants were advised to signal by raising their hand if they experienced any discomfort or dizziness during the session. Participants wore a Head Mounted Display (HMD) device and used a controller to interact with the content under the trainer’s guidance. To prevent injuries from potential dizziness, they remained seated throughout the training sessions (Fig. 2). The training was paused whenever a participant raised their hand. Those who stopped were given time to rest and stabilize. Meanwhile, the trainer demonstrated the activities, allowing participants to watch and follow along. For the AR training, the content was downloaded onto a tablet computer, enabling participants to engage with the training by observing and mimicking the voice and movements of an avatar presented in the content (Fig. 3).
3. Instruments
The pretest was conducted after obtaining consent and before the participants started the program, while the posttest was carried out three days following the program’s completion.
To ensure the groups were comparable, we used a self-administered questionnaire to gather information on the general characteristics of the subjects, such as gender, age, education level, economic status, and whether they lived with a spouse. The Korean version of the Mini-Mental Status Examination (MMSE-K) [18] was employed to assess cognitive function. The MMSE-K is comprised of seven sections: attention and calculation (5 points), memory recall (3 points), language (8 points), memory registration (3 points), spatial orientation (5 points), time orientation (5 points), and visual construction (1 point), yielding a total possible score of 30 points. Higher scores indicate better cognitive function, with scores above 24 points considered within the normal range. Oral health-related behaviors surveyed included the frequency of toothbrushing, tongue cleaning, gum cleaning, use of oral hygiene products, use of toothpicks, and whether the participants had undergone scaling in the past six months.
Oral health was assessed before and after the training to evaluate the effectiveness of the oral strength training program. To do this, we utilized questionnaires to measure the Oral Health Impact Profile (OHIP) and the Geriatric Oral Health Assessment Index (GOHAI). Additionally, oral examinations were conducted by a single researcher for each area, ensuring consistency by including the same items in both the pretest and posttest assessments.
The oral condition was assessed by applying a tooth colorant (Trace®, Young Dental, USA) to the mesial, distal, buccal, and lingual surfaces and using the O’Leary index [19] to evaluate the presence of bacterial film. A score of 1 indicated the presence of a bacterial film, while a score of 0 indicated its absence, with lower scores signifying lesser bacterial film presence. Tongue plaque was evaluated using the Winkel Tongue Coating Index [20] by dividing the tongue into three transverse sections and two sections from the root to the tip, totaling six sections. A score of 1 was assigned for the presence of tongue plaque and 0 for its absence, with a higher score suggesting more tongue plaque. The status of gingivitis was determined using the gingivitis index by Löe & Silness [21], assessing inflammation on the mesial, distal, buccal, and lingual surfaces. The scores ranged from 0 for no inflammation to 3 for severe inflammation, with lower scores indicating healthier gums. To measure the non-stimulated salivary flow rate (SFR), participants were first asked to swallow any saliva in their mouths and then, after keeping their mouths closed for 5 minutes, to spit the naturally pooled saliva into a test tube [22]. Saliva volume was measured by weight (g), equating 1 mL to approximately 1 g, with higher values indicating increased salivation. Oral muscle strength was measured using the Iowa Oral Performance Instrument (IOPI) (IOPI Medical, WA, USA) for both anterior and posterior tongue and cheek muscle strength [23]. For anterior tongue strength, the IOPI bulb was placed 10 mm anterior to the tongue at the alveolar ridge of the hard palate. Posterior tongue strength was measured by placing the bulb at the back of the hard palate, with participants pressing against the bulb with maximum force for 2 seconds. Cheek strength was assessed by positioning the bulb between the teeth and the medial aspect of the cheek, with participants squeezing the bulb with maximum effort for 2 seconds. Higher numbers indicated stronger oral muscle strength.
4. Data analysis
The collected data were analyzed using IBM SPSS Statistics (version 22.0; IBM Corp., Armonk, NY, USA), with the statistical significance level set at 0.05. Fisher’s exact test and the chi-square test were employed to compare the general characteristics and oral health behavior of the participants. The mean values of cognitive function were assessed for homogeneity between groups using an independent samples t-test. To evaluate the differences before and after the intervention, a paired t-test was used, and an independent t-test was utilized to compare the post-treatment results between groups after ensuring baseline homogeneity.
Results
1. Participants’ general characteristics
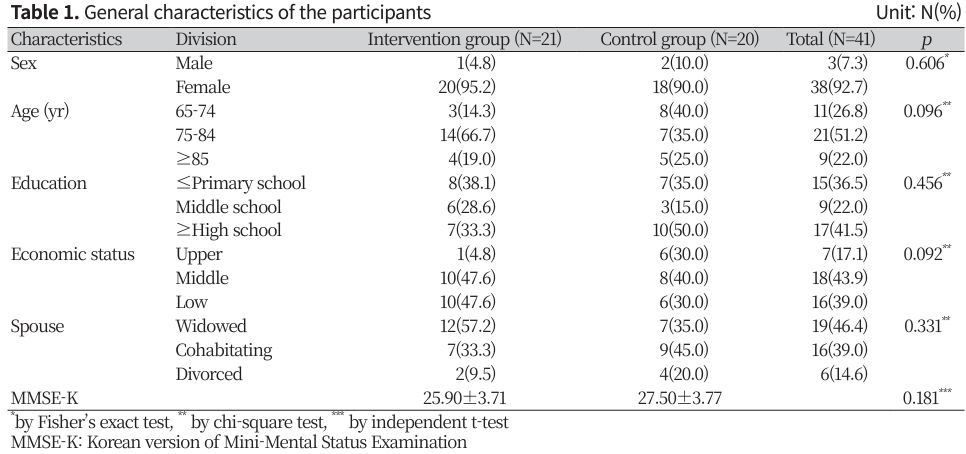
The general characteristics examined included gender, age, education level, economic status, spousal cohabitation status, and MMSE-K scores. There were no statistically significant differences between the two groups at baseline. There was a higher percentage of females compared to males, with the most common age group being 75-84 years. In the experimental group, the majority had an education level of elementary school or lower, identified as middle class, and were widowed. The average MMSE-K scores were 25.90 for the experimental group and 27.50 for the control group, both within the normal range (Table 1).
2. Oral health-related behavioral characteristics
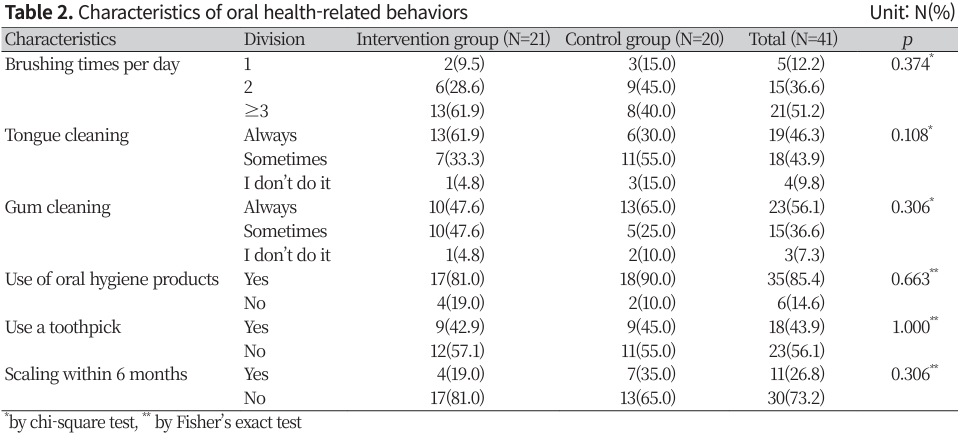
The oral health-related behavioral characteristics examined included the frequency of brushing, tongue cleaning, gum cleaning, the use of oral hygiene products, toothpick use, and whether participants had undergone scaling in the last six months. There were no statistically significant differences between the two groups at baseline. Participants in both groups were most likely to brush their teeth at least three times a day, consistently clean their tongue and gums, use oral hygiene products, refrain from using toothpicks, and not have undergone scaling in the past six months (Table 2).
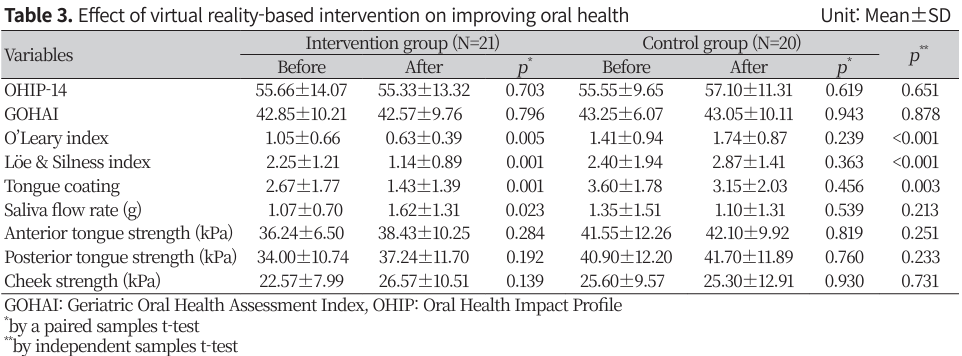
3. Effects of VR-based oral strength training in improving oral function
The O’Leary index decreased by 0.42 points (p<0.01), and the gingivitis index (Löe & Silness) decreased by 1.11 points (p<0.01). Additionally, tongue plaque reduced by 1.24 points (p<0.01), while salivation increased by 0.55 grams (p<0.05). Post-hoc comparisons between the two groups revealed significant differences in gingival bacterial film (p<0.001), gingivitis (p<0.001), and tongue plaque (p<0.01). Although oral muscle strength improved in the posttest compared to baseline, this improvement was not statistically significant. There were minimal changes in the OHIP and the GOHAI (Table 3).
Discussion
Learning with VR technology can be more engaging because it immerses learners in a virtual environment, creating memorable experiences by engaging both visual and kinesthetic nerves. This combination of physical activity with cognitive learning content can make the learning process more effective [24]. However, as this method diverges from traditional education, the general public, especially older adults, might have limited knowledge about VR-based learning. Specifically, older adults might face challenges accessing or using digital technology, leading to potential negative perceptions of VR. Previous research [16] has shown that older adults may experience psychological barriers when approaching new media. Nevertheless, VR technologies have been evolving, with HMDs becoming lighter and more user-friendly and thus also becoming more accessible to older adults. In light of these developments, we created oral strength training programs utilizing both VR and AR technologies and evaluated their effectiveness in improving oral function among older adults.
After the training, participants exhibited reductions in bacterial film, gingivitis, and tongue plaque, findings that align with those from a comprehensive oral exercise program for older adults [25], which also reported decreases in bacterial film and gingivitis. Additionally, an increase in salivation was observed, marking a significant outcome. Many older adults face problems such as bad breath, tooth decay, and, in severe cases, ulcers and oral mucosa burning due to decreased salivation [26]. Studies have indicated that oral intervention programs, including tongue exercises, can lead to an increase in salivation [27], a result that mirrors the outcomes of this study. The reduction in bacterial film, gingivitis, and tongue plaque may also be linked to the increase in salivation. Saliva is vital for oral health as it serves as an antibacterial agent, buffers pH, and protects both teeth and oral mucosa [28]. Thus, the enhanced salivary secretion likely played a role in reducing inflammation and improving oral hygiene.
Masticatory function is closely linked to oral muscle strength [29], highlighting the importance for older adults to strengthen their oral muscles early on to maintain a healthy lifestyle. However, this study did not find a significant improvement in oral muscle strength following the program, a finding that contradicts previous research [3-7]. This discrepancy might be due to the relatively short duration of the training program (6 weeks). Changes in indicators like gingival bacterial film, gingivitis, and tongue plaque can become evident within a short timeframe, but improvements in oral muscle strength, which involves muscle development, may not manifest as rapidly. This suggests a need for further research over longer periods to fully understand the impact of training on oral muscle strength. Additionally, minimal changes were observed in the OHIP and GOHAI, indicating that improvements in subjective oral health quality of life might also require longer periods to become apparent.
This study utilized a non-probability sampling method to recruit a small number of participants from a select few locations, warranting caution when generalizing the results. Some older participants faced challenges with direct manipulation and engaged in the training indirectly through observation, which complicates the evaluation of VR-based training’s effectiveness. A direct comparison of our results with existing literature was not feasible due to the scarcity of similar studies both in Korea and internationally. Although we observed positive changes in oral muscle strength, these changes were not statistically significant. Despite this, our findings are important as they demonstrate the feasibility of implementing VR-based educational content for older adults and confirm that VR-based oral muscle strength training can enhance oral health. Future research should aim to include a larger study population and undertake longitudinal studies to assess the long-term retention and evolution of the effects, thereby providing a stronger validation of the content and training methods.
Conclusions
This study aimed to develop VR-based oral strength training content and apply it to older adults to assess the effectiveness of improving oral function.
The oral strength training was conducted 12 times over 6 weeks period from late August to early October 2023. Sessions took place at the participants’ institutions, with each session lasting approximately 60 minutes. The study yielded the following results:
1. The O’Leary index decreased by 0.42 points (p<0.01), and the Löe & Silness index decreased by 1.11 points (p<0.01) following the VR-based oral muscle strength training. Tongue tie decreased by 1.24 points (p<0.01), and salivation increased by 0.55 grams (p<0.05). Post hoc comparisons between the two groups revealed significant differences in gingival bacterial film (p<0.001), gingivitis (p<0.001), and tongue plaque (p<0.01).
The outcomes of this study indicate that VR-based oral strength training can improve oral health among older adults. Therefore, the VR-based oral strength training content developed in this study could be beneficial in health promotion programs for the elderly.
Notes
Author Contributions
Conceptualization: KH Lee, YY Choi; Data collection: HY Moon, KJ Lee. MS Yoon; Formal analysis: ES Jung; Writing-original draft: KH Lee; Writing-review&editing: YY Choi, ES Jung , KJ Lee , HY Moon , MS Yoon, KH Lee
Conflicts of Interest
The authors declared no conflicts of interest.
Funding
This work was supported by the National Research Foundation of Korea (No. 2022R1A2C2010905) and funded by the government (Ministry of Science and ICT).
Ethical Statement
The Institutional Review Board (IRB approval number: SHIRB-202403-HR-224-02) approved the study, ensuring ethical protection for the participants.
Acknowledgements
None.

