Introduction
With a declining birth rate and a rapidly aged society, Korea has the highest growth rate in health expenditure in the Organisation for Economic Co-operation and Development (OECD). Public health insurance coverage in Korea is very low, and although insurance operations and finances are concentrated in the central government, medical care is highly dependent on the private sector. Due to the lack of control and management of uninsured medical care services, the burden of medical costs is expected to increase in the future [1].
According to the survey on medical expenses for health insurance patients, the health insurance coverage rate is 25.6% for dental hospitals and 36.0% for dental clinics, which is very low compared to other medical facilities, resulting in high patient burden [2]. The patient burden is higher than in other countries, which may lead to health inequalities based on socioeconomic status. In particular, children’s oral health is strongly influenced by where they live and by their parents, so providing more preventive dental services to children could improve oral health and reduce costs [3].
Previous studies have shown that health is unequal across socioeconomic levels [4], and oral health is also inversely correlated with the Decayed, Missing and Filled Teeth Index (DMFT Index) in 12-year-old children and the ratio of health and medical budget to national income per capita [5]. In 2009, dental sealants were included in the health insurance coverage as a preventive service, but this still focused on treatment rather than preventive comprehensive oral health care, which is very important for oral disease management [6].
In recent years, the government has repeatedly called for the introduction of a national primary care system to improve the efficiency of the healthcare system. This system can improve people’s health and raise the level of primary healthcare services. It is also known to be beneficial to residents and the government by increasing health insurance coverage and reducing health care costs [7]. The dental primary care scheme prioritizes the promotion of preventive oral health. It is expected to achieve greater results when targeted at children, who are most likely to benefit. With this expectation, developed countries are already providing dental care for children and adolescents [8].
In the US, the Patient-Centered Medical Home (PCMH) reports that early preventive dental care improves oral health, and the American Academy of Pediatric Dentistry (AAPD) reports that it provides cost-effective, high-quality dental services [9]. However, the UK’s the new dental contract reform: prototypes overview document reported that although the program improved oral health by preventing caries and periodontal disease in patients, it did not achieve its aims because this activity carried out over smaller number of patients and fewer treatment [10].
A recent evaluation of the governance of the student dental primary care program in Seoul [11], it requires joint efforts and consensus among professionals, including not only dentists but also dental hygienists’ associations and academics, and that dental hygienists should share the need and purpose of the program and become stakeholders in the provision of oral health services, rather than simply participants who receive the program. Dental hygienists are professionals who provide education to prevent oral disease and promote oral health, and their role in dental care service is important. Students, as future dental hygienists, need to understand the role and needs of dental hygienists in primary dental care. Therefore, the study population included dental hygienists, students and dentists interested in the children’s dental primary care program.
Methods
1. Subjects
A total of 145 dental hygienists, students, and dentists in Jeollanam-do were included in the study. This study was approved by the Institutional Review Board the of C College (CA17-211228-HR-002-01) and was conducted online for a total of 4 weeks from July 2022. The minimum sample size was calculated to be 116. Using the G*power program [12,13], a significance level of 0.05, a power of 80%, an odds ratio of 0.77 for the comparison reference group in the previous study and an expected ratio of 0.5 for the comparison target group in this study were calculated, and the method of analysis was the chi-squared test. Assuming a dropout rate of 20%, 124 subjects were eligible for analysis. The ratio for the comparison group was based on the results of the needs assessment of the primary care program in a previous study [14].
2. Methods
stionnaire consisted of 16 items, including 4 items on the general characteristics of the study population, 4 items on the need for services, 4 items on the importance of the services and 4 items on the frequency of service provision. The need for services was multi-response, the importance of services was based on a 5-point Likert scale, and the frequency of service provision was selected from 3, 6, and 12 months. The questionnaire was adapted from Choi’s study [15] and modified for this study.
3. Analysis method
The data collected were analysed using SPSS 18.0. Independent t-test and ANOVA were used to compare differences in the roles and needs of dental hygienists according to general characteristics, and correlations were analysed. Post hoc tests were analysed using Scheffé‘s test. In addition, to check the internal reliability of the questions, Cronbach’s alpha was calculated and was 0.850 for oral examination, 0.846 for oral health education, 0.848 for preventive treatment and 0.867 for dental treatment.
Results
1. General characters of study subjects
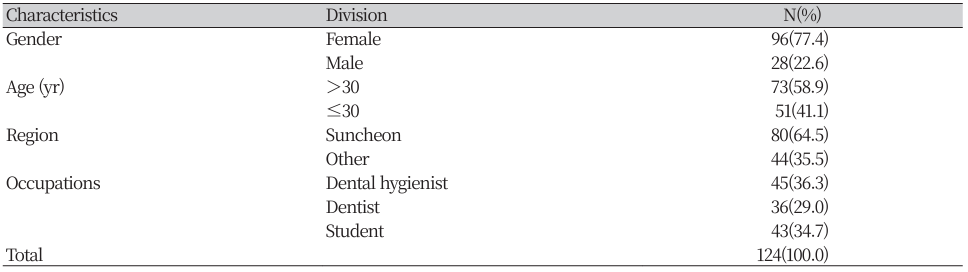
The general characteristics of the study participants are shown in (Table 1). The final number of subjects was 124, excluding 21 who did not complete the questionnaire. 77.4% were female and most were in their 20’s (58.9%). 64.5% were from Suncheon and 36.3% were dental hygienists.
2. Essential services, importance, period of service, and providers by variable
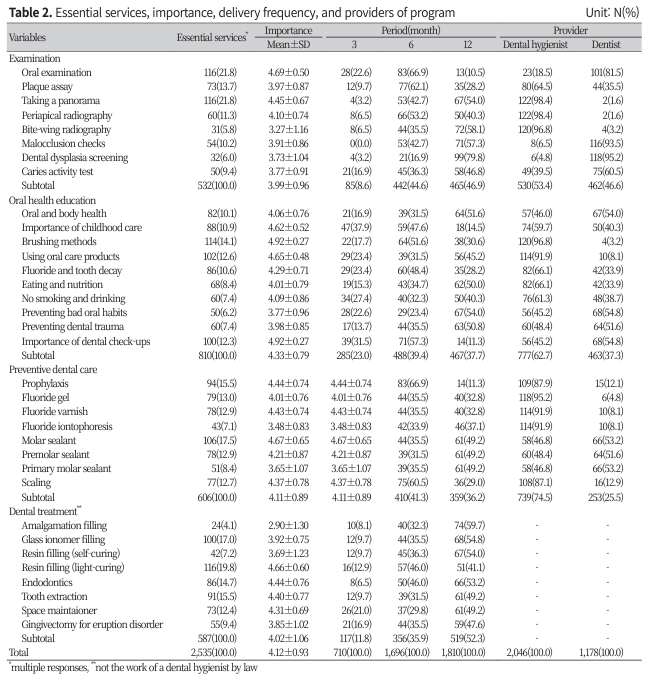
As shown in (Table 2), oral examination (21.8%) and panoramic radiographs (21.8%) were high on the list of essential services, whereas bitewing radiographs (5.8%) and screening for dysplasia (6.0%) were low. In oral health education, people were more likely to be taught how to brush their teeth (14.1%), how to use oral products (12.6%) and the importance of regular dental check-ups (12.3%), and less likely to be taught how to prevent bad oral habits (6.2%), how to stop drinking and smoking (7.4%) and how to prevent dental trauma (7.4%). In terms of preventive dental care, molar sealants (17.5%) and prophylaxis (15.5%) were high, while fluoride iontophoresis (7.1%) and primary molar sealants (8.4%) were low. In dental treatment, light-curing resin fillings (19.8%) and glass ionomer(GI) fillings (17.0%) were high, while amalgam fillings (4.1%) and self-curing resin fillings (7.2%) were low.
The importance of oral examination items was high for oral examination (4.69 points) and panoramic radiograph (4.45 points), but low for bitewing radiograph (3.27 points) and screening for dysplasia (3.73 points). The importance of oral health education was high for tooth brushing methods (4.92 points) and dental check-ups (4.92 points), but low for prevention of bad oral habits (3.77 points) and prevention of dental trauma (3.98 points). In preventive care, molar sealants (4.67 points) and oral prophylaxis (4.44 points) scored high, while fluoride iontophoresis (3.48 points) and primary molar sealants (3.65 points) scored low. In dental treatment, light-curing resin fillings (4.66 points) and endodontics (4.44 points) were high, while amalgam fillings (2.9 points) and self-curing resin fillings (3.69 points) were low.
Examination intervals were more likely to be 12 months (46.9%) or 6 months (44.6%), oral health education intervals were more likely to be 6 months (39.4%) and 12 months (37.7%), and preventive care intervals were more likely to be 6 months (41.3%) and 12 months (36.1%), but treatment intervals were more likely to be 12 months (41.3%).
Radiographs (96.8-98.4%) and plaque assay (64.5%) were considered appropriate by dental hygienists, whereas dentists dental considered dysplasia screening (95.2%), malocclusion checks (93.5%), oral examination (81.5%), and caries activity test (60.5%) appropriate. Oral health education (62.7%) and preventive care (74.5%) were more likely to be provided by dental hygienists. Dental treatment is not performed by dental hygienists, so it was not investigated and analysed.
3. Differences in the importance of subprogram by general characteristics
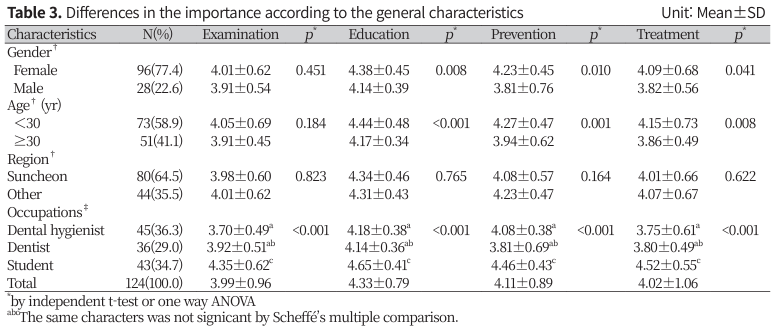
There were statistically significant differences in oral examination, education, prevention and treatment according to the general characteristics of the study population (Table 3). Females rated education (P<0.01), prevention (P<0.05), and treatment (P<0.05) higher than males, and those over 30 years of age rated education (P<0.01), prevention (P<0.01), and treatment (P<0.01) higher than those under 30 years of age, and the differences by region were not statistically significant. There were statistically significant differences in examination (P<0.01), education (P<0.01), prevention (P<0.01), and treatment (P<0.01) by occupation. Students rated the importance of examination, education and prevention in the program higher than dental hygienists and dentists. The importance of treatment was also higher among students.
6. Correlation between variables in the importance
(Table 4) shows the correlation between the importance of oral examination, education, prevention, and treatment. As the importance of examination increased, the importance of education (α=0.826), prevention (α=0.606), and treatment (α=0.714) also increased (P<0.01). In particular, there was a high correlation between the importance of examination and that of education. The importance of oral health education also increased, as did has the intensity of prevention (α=0.536), treatment (α=0.611), and oral examinations(α=0.826, P<0.01). That of prevention increased, as did that of the examination (α=0.606), the education (α=0.536), and the treatment (α=0.740, P<0.01). In addition, the higher that of the treatment, the higher that of the examination (α=0.714), the the education (α=0.611), and the treatment (α=0.740, P<0.01).
(Table 5) shows the correlation between essential service and importance of oral examination, education, preventive dental care, and dental treatment. Higher importance was associated with higher need (α=0.447, P<0.001).

Discussion
The researcher identified the role and needs of dental hygienists in the program which provides primary dental care for children.
In terms of service needs, oral examinations and panoramic radiographs were considered essential, oral health education should include education on brushing, the use of oral products, and the importance of regular examinations, and preventive care such as molar sealants and prophylaxis was needed. There was also a high need for light-curing resins and GI fillings in dental care. Choi [15] also reported that examinations(history taking and oral inspection), and panoramic radiographs were the most needed for examination, and that brushing and education on childhood oral health care were important. For prophylaxis, molar sealants and oral prophylaxis were indicated. Treatment included composite resin fillings and tooth extractions.
According to the Standard Service Manual for Family Dentists for Children [8], the oral examination includes history taking and inspection, caries risk assessment (biological predisposing factors, prophylactic factors, and clinical observation), and plaque scoring (PHP index) as mandatory services, and panoramic photography as an optional service if necessary. Mandatory education included the importance of childhood oral health care, the relationship between oral and systemic health, brushing and flossing, fluoride application, diet and nutrition, and optional education service included the use of oral care products. Mandatory preventive services included prophylaxis and fluoride varnish, and sealants were optional. Treatment services such as fillings, endodontic treatment, extractions and space maintainers were also optional. The policy evaluation of dentist system for Seoul’s student and children [3] also reported that education on dietary habits, smoking cessation and temperance was provided somewhat less than education on oral hygiene management such as brushing and flossing and fluoride use.
In terms of examination, oral examinations and panoramic radiographs were considered important, but bitewing radiographs and screening for dysplasia were not considered relatively unimportant. In education, brushing techniques and regular check-ups were considered important, but bad oral habits and prevention of dental trauma were relatively unimportant. The most important preventive treatments were molar sealants and oral prophylaxis, while fluoride iontophoresis and primary molar sealants were less important. light-curing resin fillings and root canal treatment were important, while amalgam fillings and self-curing resin fillings were not. Choi [15] reported similar importance of oral examinations, education, preventive care, and treatment services. The policy evaluation of dentist system for Seoul’s student and children [3] emphasised the importance of oral health education, including tooth brushing, and stated that for the system to be successful, it is very important that not only children but also their parents have oral health knowledge, awareness of prevention, and especially that adults’ oral health affects their children, and that it is very important to warn them to pay attention to and take care of their children’s oral health. The importance and effectiveness of smoking cessation and sobriety was also highlighted, as it was only offered to less than half of the students screened. In the United States, Medicaid and the Children’s Health Insurance Programme (CHIP) provide routine oral examinations and radiographs, as well as preventive, educational, filling, endodontic, periodontal, prosthodontic, and oral and maxillofacial surgery services; in Canada, the healthy smile ontario program provides examination, diagnosis, prevention, and treatment as core services, preventive services, and emergency and essential services [16,17].
The frequency of follow-up was 6 months for education and prevention and 12 months for treatment, with education and prevention requiring more frequent follow-up than treatment. Choi [15] reported a 6-month cycle for oral examination, education, and prevention, and did not investigated treatment services; however, she reported that a 12-month cycle was appropriate for panoramic photography and malocclusion screening in oral examination, and for education on the relationship between oral and systemic health, smoking cessation and sobriety, prevention of dental trauma, and prophylaxis for dental calculus removal. The standard service manual for family dentists for children [8] and the American Academy of Pediatric Dentistry [16] recommended a 6 month follow-up interval, with three months for high-risk groups.The Seoul Metropolitan Government provides oral examinations, education, and preventive services to participating students once a year at a cost of 40,000 won per student through a private dental clinic that has signed a business agreement with the Korean Dental Association. France requires mandatory annual oral examinations and free dental treatment within nine months of the examination [18]. In the United States, the timeframe varies from state to state, but in Washington state, major examinations and preventive care are recommended three to four times a year, with those eligible are expected to pay around $7 to $20. Canada offers free annual examination, prevention, and treatment services if those meet household income guidelines [16,19].Radiographs and plaque assay were considered appropriate by dental hygienists, while dental dysplasia screening, malocclusion checks, oral examination, and caries activity test appropriate by dentists. Dental hygienists were more likely to provide oral health education and preventive care. According to the Act and its the implementing legislation [20], dental hygienists are required to ligate and remove orthodontic wire, apply fluoride, take diagnostic radiographs, perform temporary fillings, cement and remove temporary attachments, perform scaling and oral prophylaxis, take dental impressions, and provide other dental and oral disease prevention and hygiene care. According to the standard service manual for family dentists for children [8], professional care should be provided by a dental hygienist for education service and a dentist or dental hygienist for preventive services.There were statistically significant differences in the importance of screening, education, prevention, and treatment services based on the general characteristics of the study population. The importance of education, prevention, and treatment services was higher for female than for male and for those aged 30 years and over than for those aged younger than 30 years, with no statistically significant differences by region. Dental hygiene students were also more likely to use examination, education, prevention, and treatment services than dental hygienists and dentists. This difference may be due to the fact that dental hygiene students feeling that what they learned in law or in school was different from their experience in practice. Previous studies [21,22] have shown that dental hygiene students perceive dentists that dentists perform different task or that the division of labour is not clear. They also have different perceptions of the detailed scope of dental hygienists’ duties, including oral examination, education, asisting, and administration and management.Oral examinations were positively correlated with education, prevention, and treatment services. In particular, examinations were highly correlated with education and treatment, and prevention and treatment, so it is necessary to follow up examinations regularly with education, prevention, or treatment services. Participation in the study was also positively correlated with the importance of the essential services of a child’s family dentistry program. A study by Shun and Choi [23] found that people of all ages who have not had an oral examination are at high risk of oral disease and have high treatment costs, so ongoing care and screening are important for early caries and prevention. To prevent and care a early childhood caries (ECC), infants and young children should receive oral examinations, and lifelong health care strategies and early screening are needed [24].This study focused on dental hygienists and dentists, who are essential staff in a children’s family dentistry program, and also on students who are future dental hygienists. It is useful to analyse the needs of the program by investigating the essential services to be provided, their importance, period of service, and who should be the appropriate providers, so that it can be used as a basic data for the development and operation of future programs. However, a limitation of the study was that it was not generalisable as it was carried out in a small geographical area. Further research is needed to study the demand and need for the program by including members of the pilot Children’s Family Dentistry Program.Conclusions
Researchers have identified the following essential service needed in a children’s family dentistry program, their importance, period of service, and the role of the dental hygienist.
1. Oral examination and panoramic radiography are an essential part of the examination. Oral health education should include brushing, use of oral products, and the importance of regular examination, preventive service such as molar sealants and prophylaxis are necessary. And treatments such as light-curing resin and GI filling are essential.
2. The frequency of assessment is 6 months for education and prevention and 12 months for treatment, with education and prevention being more frequent than treatment.
3. Dental hygiene students feel that examination, education, prevention, and treatment services are more important than dental hygienists and dentists.
4. Oral examinations are highly correlated with education and treatment, and prevention and treatment, and are positively correlated with the essential services and thier importance.
Children’s family dentistry program should provide services that are considered necessary and important. Examination and education should be more frequent than treatment, and the importance of the program should be emphasised not only to dental hygiene students but also to the dental hygienists and dentists who are integral to the program.

